Rewriting Life
A Change of Mind
Diana Bianchi championed tests that find Down syndrome early in pregnancy. Now can she find a way to treat it?

Diana Bianchi leads a search for drugs that could treat Down syndrome.

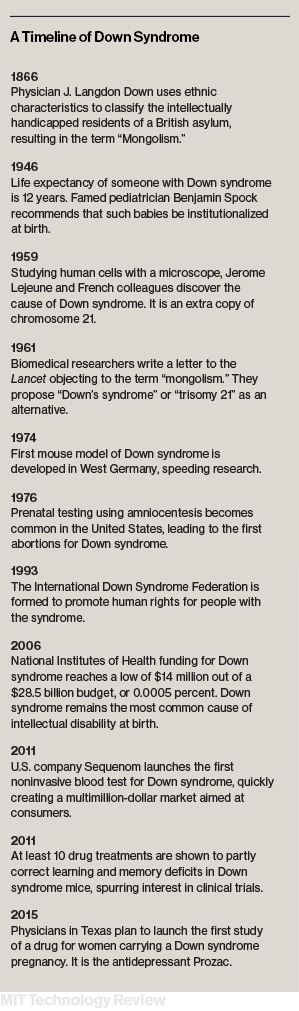
Jerome Lejeune is the Frenchman who discovered the chromosomal error responsible for causing Down syndrome, half a century ago. Lejeune, who died in 1994, was a devout Catholic, and he was aghast when he realized his discovery would lead to prenatal tests and abortions. In his view, this was eliminating the patients instead of treating them. Someday, he felt certain, a cure would be found. “We will beat this disease,” he wrote. “It’s inconceivable that we won’t. It will take much less intellectual effort than sending a man to the Moon.”
A framed letter from Lejeune hangs outside the office of Diana Bianchi, who is arguably America’s best-known neonatal geneticist. She is celebrated because of the role she’s played in introducing noninvasive prenatal testing and documenting its accuracy and drawbacks (see 10 Breakthrough Technologies 2013: “Prenatal DNA Sequencing”). The blood tests she researches are an improved way to detect chromosomal disorders such as Down syndrome, also called trisomy 21, the most common genetic birth defect causing intellectual disability. Since the tests debuted in 2011, according to calculations from Bianchi’s research institute for maternal and fetal medicine at Tufts Medical Center, more than two million have been performed.
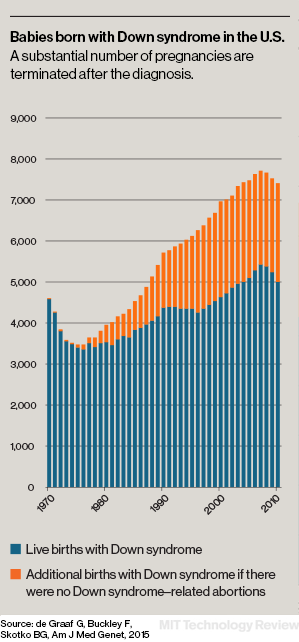
The tests are highly accurate and can detect Down syndrome as early as the first trimester. But the medical options in the face of a positive result remain as starkly limited as they were in Lejeune’s day: continue the pregnancy and have a child with multiple disabilities, or don’t. Sixty to 70 percent of women who receive a prenatal diagnosis of Down syndrome in the United States opt for abortion, according to a peer-reviewed article in the journal Prenatal Diagnosis.
That’s why Bianchi’s role in the rapid spread of noninvasive testing has also made her the target of critics, particularly people with Down syndrome and their parents, who say they are happy as they are. To those who have posted criticisms of Bianchi on the Web or personal attacks on her hospital’s Facebook page, the goal of improved tests can only be fewer people with Down syndrome.
To those who will listen, though, Bianchi has been advancing an entirely different scenario. She says that early testing will lead to the first treatments for Down syndrome. With the ability to routinely detect the syndrome as early as 10 weeks of pregnancy, she says, the tests are creating the chance to develop drugs that address cognitive deficits in the womb. “Plenty of people think that their children with Down syndrome are perfect the way they are,” says Bianchi. “But there are also plenty of people who, if given the choice, would want to attempt to treat their children.” Critics of testing “don’t know the complete picture,” she says. “They don’t realize there is another half to the equation.”
On the day I visited Bianchi at her lab in Boston’s Chinatown, she was wearing a soft teal turtleneck and a taupe blazer. She guided me to her lab, where we slipped on gauzy elasticized hair coverings, long-sleeved gowns, booties, and gloves before viewing brown mice, some with a condition mimicking Down syndrome. Some of their mothers had been treated with a common drug or supplement (Bianchi said it’s possible they could ultimately test combinations of drugs, but for now they’re testing them one by one). It’s an attempt to enhance the growth of the young mice’s neurons during a critical stage of brain development.
Bianchi’s drug search remains a relatively small effort, focused on safe and already-approved drugs that could be used in utero. Others are also beginning to look at treatments. A Texas hospital is readying a trial of Prozac in pregnant women whose fetuses have Down syndrome, and a scientist at Cornell is investigating supplementation with choline, an essential nutrient. This past summer in Paris, Bianchi led what she calls a “really historic” session at the Trisomy 21 Research Society meeting, devoted to prenatal treatments. Just stirring interest in treatment feels like a fairly big achievement, she says.
Bianchi, now 60, was a college student in 1973 when she wrote to Lejeune to ask for an internship. She says she forgot about the correspondence until 2012, when she unearthed a handwritten response from him that she’d tucked away in a box four decades ago—the one now displayed outside her office. In it, Lejeune complimented her French and offered his “cordial sympathies” that there was no place in his lab. She says rediscovering the letter as she began working on a treatment felt symbolic: “I thought, ‘This is a sign.’ It shows that I have been thinking about this for a while. It was a sign that this was meant to be.”
One convert to Bianchi’s campaign is Mark Bradford, father of a son with Down syndrome and president of the Jerome Lejeune Foundation USA, the American arm of a Paris-based group. He says the foundation’s view remains that noninvasive prenatal testing is “an incredible threat to the Down syndrome community,” but he has come to believe that Bianchi will develop “an antidote” to that threat and is helping to fund her search for a drug. Bianchi says Bradford was the first member of the polarized Down syndrome community to listen to her ideas. “I think one day she will prove to have been a heroine in that her advancement of [noninvasive tests] will be the gateway to early therapy and will save countless lives,” says Bradford. “She is very unjustly and harshly criticized for her work by people who can’t see [past] prenatal diagnosis to its future benefit.”
Early as possible
The nucleus of a normal human cell contains 46 chromosomes. But in people with Down syndrome there are 47: an error that occurs in sperm or egg cells before fertilization results in an added copy of the 21st chromosome. The extra chromosome, which harbors more than 200 protein-coding genes, is transmitted to every cell in a person’s body. That results in intellectual delays, heart problems, and other conditions that shorten life span, and physical features such as eyes that slant upward. The pervasive nature of the disorder is what’s always made it difficult to imagine how it could be treated.
And for a very long time, scientists stopped wondering. They worked on better tests to detect the disorder prenatally, but as Bianchi acknowledges, they paid virtually no attention to what was actually occurring in Down syndrome pregnancies. Bianchi now thinks there is a window of opportunity when the brain development of a fetus with Down syndrome begins to diverge from the normal path. At about 15 weeks of pregnancy, she says, the brain starts to grow more slowly than usual. In the most severe cases, the fully developed brain can end up 75 percent as big as that of a typical newborn. Perhaps this slowdown could be minimized if the mother were given the appropriate drug as soon as a diagnosis was made. “You want to address the problem as early as it can be detected,” says Tarik Haydar, who runs the Laboratory of Neural Development and Intellectual Disorders at Boston University and collaborates with Bianchi.
Neurogenesis—the creation of neurons—occurs largely in the womb. Between birth and puberty, neurons mature and go through a process of myelination, or insulation, and formation of synapses, or connections. Neurogenesis continues too, but at a snail’s pace compared with the rapid-fire production in the womb, where—on average—300 million neurons are created per day in early pregnancy. “There is still something you can do after birth, but if you really hope to rescue neurogenesis, you have to do it prenatally,” says Renata Bartesaghi, a professor in the Department of Biomedical and Neuromotor Sciences at the University of Bologna.
Bianchi has called this possibility “fetal personalized medicine.” Any kind of fetal medicine is still very unusual, though. There are a few complex fetal surgeries to repair birth defects, but only one drug, the vitamin folic acid, is taken regularly to steer the course of prenatal development. If women have the supplement in their bodies from conception through the first weeks of pregnancy, their babies are protected from neural tube defects including spina bifida, a malformation of the spinal cord. Folic acid points to the importance of timing. If taken at the right time, it prevents a serious error in development. But no amount of folic acid will help after development has run its course.
Bianchi began testing drugs for Down syndrome on mice in 2011, theorizing that it might be possible to change the brains of babies with something as simple as folic acid. Her thinking had changed when she learned of efforts to treat fragile X syndrome, another cause of intellectual impairment, and as new tools to investigate development became available—including the noninvasive tests, which launched that year. “I realized that research in neurocognition was changing rapidly,” she says.

The physical differences in Down syndrome can be seen in an ultrasound: more fluid accumulation at the back of the neck, or an absent nasal bone. But one of Bianchi’s first steps was to try to find a molecular signature of the disorder by collecting amniotic fluid from pregnant women, in order to measure the “transcriptome” of fetal cells—a readout of which genes are turned on or off. She found about 300 genes that behaved differently in Down syndrome, and most of them were not on chromosome 21. That underscored the complexity of the disease, but it also provided what Bianchi says is her key finding. The gene patterns in fetuses with Down syndrome suggested high levels of oxidative stress, an indication that cells were being damaged. “We all have oxidative stress,” says Bianchi, “but our systems take care of it. Is there more in a Down syndrome fetus, or can they just not handle it?” Bianchi’s hypothesis is that the abnormal biochemical environment is knocking out stem cells that would otherwise be making new neurons.
Bianchi has been searching for drugs that can reduce oxidative stress and possibly “rescue” neurogenesis, at least in part. It is the sort of early-stage prospecting that a drug company might do, if any were pursuing a prenatal therapy for Down syndrome. Her search has been very conservative, restricted to drugs that are already sold for other purposes and have good safety records. Her team located candidate drugs using a database maintained at another Boston-area research center, the Broad Institute, which holds records of how 1,300 different compounds affect the transcriptome of human cells grown in the laboratory. That database kicked out lists of compounds whose effects on gene activity are essentially the reverse of what’s seen in Down syndrome and might counteract it.
From those 1,300 drugs and chemicals, Bianchi’s group narrowed the list to 10. In her lab, the compounds are mixed into food and fed to mice, including pregnant females carrying pups, about half of whom have a condition that mimics Down syndrome.
Bianchi and postdoctoral researcher Faycal Guedj demonstrated for me how they test seven-day-old mice, some healthy and others with the rodent version of Down syndrome (the researchers conceal from themselves which are which). With a gloved hand, Guedj catches a brownish mouse that seems unusually small, just 53 millimeters.
In one test, the mouse takes 17 seconds to flip from back to belly, struggling to get its right foot out from beneath its body. In another test, it musters only enough strength to hang from a metal wire for three seconds. Bianchi guesses it is a Down syndrome mouse. A second mouse manages to hold on for nearly eight seconds and deftly flips over in four. “See how quick it was,” she marvels.
Guedj, who is from Algeria, was six when his sister, Imene, was born with Down syndrome. She can’t read, and her speech is limited to a few words that she feels confident using (“I want chocolate” is a familiar sentence). Guedj wonders how Imene’s life would have been different if she’d had the option of treatment in utero. “You see your nephews and nieces growing up and her stuck at a certain level,” he says. “We missed the opportunity of treating her early.”
Radical measures
Of the 10 compounds that Guedj and Bianchi identified, two seem particularly promising. One is apigenin, which is found in plants, but Bianchi won’t yet publicly identify the other. Each has shown therapeutic, but not groundbreaking, effects. No matter how successful the drugs might be, Bianchi does not expect them to change the physical appearance of people with Down syndrome; nor is it likely that they’d reduce the incidence of heart defects, which occur in about half of babies with the disorder. “From what I’ve seen so far, there is no magic bullet where you take the drug and everyone is cured,” she says.

Some researchers, however, are contemplating more radical measures. Jeanne Lawrence, a professor in the Department of Cell and Developmental Biology at the University of Massachusetts, made headlines in 2013 when she succeeded in “silencing” the extra copy of chromosome 21 in human cells from a patient with Down syndrome. She did so by using gene editing to splice in a gene for an RNA coating that painted the extra chromosome with a molecular block so that none of its 250 genes produced any proteins.
To Lawrence, this is a first step toward a “chromosome therapy” that would make use of genetic engineering in the womb. “Multiple pathways are perturbed, and one drug is not enough to fix them,” she says. “If you can silence the 250 genes, you don’t need a drug.”
Fetal gene engineering probably remains far off. But the first prenatal tests of drugs in humans are likely to start soon. A group of physicians at University of Texas Southwestern in Dallas is on the verge of launching a small study to give fluoxetine, the generic form of Prozac, to women who have chosen to continue their Down syndrome pregnancies, and then to the children for the first two years of their lives. The idea springs from work by Bartesaghi, the researcher in Bologna, who has reported remarkable results administering fluoxetine to a different strain of mice with a condition that mimics Down syndrome. The antidepressant boosts the availability of serotonin, a neurotransmitter important in the development of neurons. In 2014 in the journal Brain, Bartesaghi reported that the affected mice had a normal number of neurons after birth and 45 days later. The mice were given a memory test. “They acted the same as normal mice,” she says. “They were perfect.”
Bianchi says the Italian mouse data are impressive, but she is concerned about giving large doses of Prozac—the trial calls for as much as 80 milligrams a day—to women who have no psychiatric disorder. Safety concerns will always be an obstacle to fetal treatment. “We would feel horrible if we came up with what’s in theory the perfect treatment and then in clinical trial it caused harm to mother and baby,” she says.
Nor can studies on mice reliably predict what will happen to a person’s brain. Melissa Parisi, chief of the Intellectual and Developmental Disabilities Branch at the National Institute of Child Health and Human Development, finds Bartesaghi’s and Bianchi’s work “very promising” but thinks a treatment could be far away. “We’ve cured ALS in mice a thousand times, but we still don’t have a treatment in humans,” says Parisi. “Humans are much more complicated.”
Help my child
When I asked Bianchi if her real goal is to decrease the rate of abortion for fetuses with Down syndrome, she deflected the question. “Our goal is to hopefully improve neurocognition and, in doing so, provide expectant couples with a message of hope,” she says. “What people decide to do with that information is their business.”
But if Bianchi or others do succeed with a drug therapy, the option would present new and complicated choices for expecting parents and for their doctors. Those who today would be inclined to have an abortion might reconsider. Other parents might question what it means to try to alter cognition.
“When you first discover you are having a baby with Down syndrome, your gut reaction is ‘This is a problem—how can we fix it?’” says Amy Julia Becker, who has a daughter, Penny, with the condition. Becker, who lives in Connecticut and writes frequently about Down syndrome, says her attitude has changed: “Penny is almost 10. I don’t see it any longer as a problem that needs fixing.” She would find it easier to support a treatment for the heart problems that affect many people with Down syndrome, but “the cognition piece? I’m kind of neutral on that,” she says. “There is a sense that cognition is more interwoven than heart defects with who you are.”

But many parents would be ready to leap for a promising drug. “I had a lot of fear that I wasn’t doing everything I could be doing,” says Liz O’Hara, an elementary school teacher from Connecticut, of her pregnancy with her son Michael, who was born in July and diagnosed prenatally with Down syndrome. She took megavitamins and choline supplements, tried acupuncture, and cut down on gluten and dairy. She decided against taking Prozac for fear of side effects, but she would have welcomed a treatment that had been well studied and declared safe. “Part of me would do anything to … I don’t want to say fix my child, but help my child,” she says.
So far, fetal therapies have been reserved for critical cases—a cardiac surgery to save a baby’s life, for example. Haydar says he and Bianchi have talked over the “significant social hurdles” of trying to intervene for any reason other than to keep the child from dying. “There’s obviously a challenge in talking about fetal therapy,” he says. “You don’t want to go playing around with a developing fetus, potentially affecting that individual and their family for the rest of their life, unless you have to do it to save the baby’s life.”
Haydar says he and Bianchi imagine how they would counsel parents. For example: A woman is informed in a doctor’s office that her fetus has Down syndrome, with its accompanying likelihood of intellectual disabilities and heart defects. Then the doctor would say: “There is a new breakthrough, a pill that will reduce the likelihood of intellectual disability by 50 percent or 80 percent,” says Haydar. “That’s the best-case scenario. But any time you enter into a conversation about prenatal anything, those conversations are touchy, because there is a vast array of feelings that people have. Diana and I talk about this a lot.”
Bianchi says she regularly receives e-mails inquiring about prenatal treatment. For people undecided about raising a child with Down syndrome, the promise of a drug that improves thinking might tip the scales in favor of continuing the pregnancy. “My hope is that it will change the conversation,” she says. “It gives the message that we are not giving up on your child, that your child has options to get better.”
Bonnie Rochman is a health and science writer in Seattle who is working on a book about how genetics is reshaping the experience of childhood.