
Business Impact
Paralyzed Again
We have the technology to dramatically increase the independence of people with spinal-cord injuries. The problem is bringing it to market and keeping it there.

One night in 1982, John Mumford was working on an avalanche patrol on an icy Colorado mountain pass when the van carrying him and two other men slid off the road and plunged over a cliff. The other guys were able to walk away, but Mumford had broken his neck. The lower half of his body was paralyzed, and though he could bend his arms at the elbows, he could no longer grasp things in his hands.
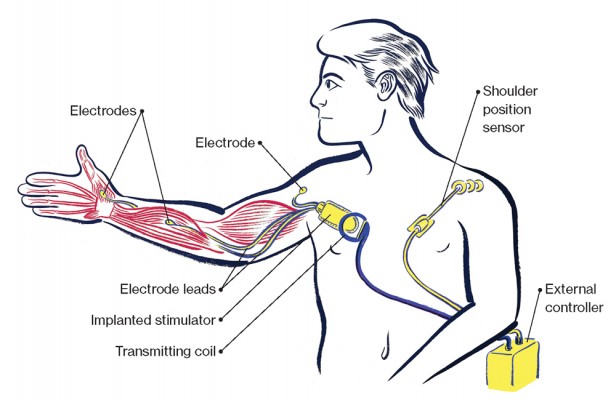
Fifteen years later, however, he received a technological wonder that reactivated his left hand. It was known as the Freehand System. A surgeon placed a sensor on Mumford’s right shoulder, implanted a pacemaker-size device known as a stimulator just below the skin on his upper chest, and threaded wires into the muscles of his left arm. On the outside of Mumford’s body, a wire ran from the shoulder sensor to an external control unit; another wire ran from that control unit to a transmitting coil over the stimulator in his chest. Out of this kludge came something incredible: by maneuvering his right shoulder in certain ways, Mumford could send signals through the stimulator and down his left arm into the muscles of his hand. The device fell short of perfection—he wished he could throw darts with his buddies. But he could hold a key or a fork or a spoon or a glass. He could open the refrigerator, take out a sandwich, and eat it on his own. Mumford was so enthusiastic that he went to work for the manufacturer, a Cleveland-area company called NeuroControl, traveling the country to demonstrate the Freehand at assistive-technology trade shows.
Mumford was in Cleveland for a marketing meeting in 2001 when he got news that still baffles him: NeuroControl was getting out of the Freehand business. It would focus instead on a bigger potential market with a device that helped stroke victims. Before long, NeuroControl went out of business entirely, wiping out at least $26 million in investment. At first, Mumford remained an enthusiastic user of the Freehand, though one thing worried him: the wires running outside his body would sometimes fray or break after catching on clothing. Each time, he found someone who could reach into his supply of replacements and reconnect the system. But by 2010, the last wire was gone, and without the prospect of tech support from NeuroControl, the electrical equipment implanted in Mumford’s body went dormant. He lost the independence that had come from having regained extensive use of one hand. “To all of a sudden have that taken away—it’s incredibly frustrating,” he says. “There’s not a day where I don’t miss it.”
Mumford’s voice rises in astonishment as he tells the tale. “I have a device implanted in my body that was considered to be one of the best innovations or inventions of that century,” he says. “The last thing you think is that the company is going to go out of business, and not only is it going to go out of business, but you’re not even going to be able to buy parts for that. That seems insane!”
Around 250 people are believed to have gotten the Freehand from NeuroControl, and Mumford was far from the only one heartbroken by the company’s failure. Their experience is a cautionary tale now for any implantable medical device that might serve “orphan markets”—relatively small groups of people. Although advances in brain-machine interfaces and electrical–stimulation devices are generating marvelous research results in people with paralysis—some are using their thoughts to control robotic arms, and others are taking tentative steps—it’s possible those breakthroughs won’t last long on the market, assuming they can be commercialized at all. Limp limbs can be reanimated by technology, but they can be quieted again by basic market economics.
The initial flourish
The technology in Mumford’s body began to be developed in the 1970s. The lead inventor, P. Hunter Peckham, a biomedical engineer at Case Western Reserve University in Cleveland, wanted to see whether electrical stimulation would reverse atrophy and ultimately restore function to paralyzed muscles. First in animals and then in people, Peckham and colleagues used hypodermic needles to inject tiny coils of wire into muscles, near nerves. They could then send mild pulses of electricity through these wires and stimulate the muscles, changing their very structure. Over time, by putting the wires in the right places and precisely tuning the bursts of electricity, the researchers could coördinate the muscles’ movements—re–creating, among other things, the normal grasp of a hand. Eventually the scientists figured out how to implant the technology into patients and let them operate it themselves, outside the lab, by means of a joystick-like unit mounted to the shoulder. The first version of what would become the Freehand system was installed in a patient in 1986. Peckham and five other investors founded NeuroControl seven years later with technologies licensed from Case Western.
When the U.S. Food and Drug Administration approved the Freehand in 1997, it was a milestone. It was not the first commercial bionic device—pacemakers and cochlear implants already existed—but it was the first that helped paralyzed patients regain some use of the hands. In fact, it was the first one that used electrical stimulation to make joints move—and to this day it remains the only one ever released.
To see how it worked, watch this promotional video made by the company in the 1990s.
Here’s Mumford marveling at the system’s power:
Independent research showed that even at a cost of around $60,000 (for the device and the necessary surgery), the Freehand saved money in the long run by reducing a patient’s need for attendant care. But while the technology was impressive, the Freehand got stuck in a small niche.
Although there are 250,000 people with spinal-cord injuries in the United States alone, the Freehand worked only for people whose paralysis stemmed from an injury to a certain area—between the fifth and sixth vertebrae of their cervical spine. That’s because a break in that location left them with enough shoulder and elbow mobility to trigger the Freehand’s grasp-and-release function. Although NeuroControl estimated its potential market at more than 50,000 people in the United States, not all of them were willing or healthy enough to endure the major operation that was required to implant the device and all those wires.
Most important, the potential market was further narrowed by the fact that some private insurers and Medicare, the U.S. government insurance program for the elderly and the disabled, would not always cover the full cost. Rehabilitation clinics and hospitals were already likely to be conservative about recommending a novel implantable system to patients. But given that they might absorb any uncovered costs from the procedure, many medical centers were more reluctant to advocate the technology than NeuroControl had hoped.
Lacking momentum, NeuroControl stopped selling the product. “The investors had expected that it would penetrate a much larger volume of the overall spinal-injury population,” says Geoff Thrope, who was NeuroControl’s director of business development. “We were able to make dozens of implant sales per year. You need to be in the hundreds, if not thousands, to have it make sense.”
But the decision still rankles Peckham, who resigned from NeuroControl’s board as a result. With some more time, he says, NeuroControl might have seen its way through to a sustainable business. It had 19 patients enrolled in a clinical trial in England; one more would have given it the 20 necessary to allow the British national health-care system to move toward covering the cost of the Freehand. The U.S. Department of Veterans Affairs was likely to follow suit, he says. The problem was that other board members—primarily venture capitalists who “decided they were not seeing the return on the investment they had anticipated”—were impatient.
“It was all legal,” Peckham says. “Whether it was ethical or not is another question. Well, I guess it depends upon what your ethics are, right?”
Wires in the warehouse
You don’t have to dig into archival footage to see the Freehand in action. A few miles from where Mumford lives in the Denver suburbs, I met Scott Abram, an accountant for the U.S. Department of the Interior. Abram broke his neck in 1989, at age 17, when he dived into a shallow river on a high school field trip. He got the Freehand a decade later and still uses it for certain tasks. When we had lunch in a restaurant, he ordered a chicken sandwich. By activating the Freehand with shrugs of his left shoulder, he was able to manipulate his right hand in ways that helped him bring the sandwich to his mouth and down to the plate. All the while, a pager-like control unit on the left side of his wheelchair was still doing what it has done for 15 years: telling the stimulator in his chest which wires in his right arm needed jolts of electricity.
Abram knows full well what Mumford went through when the wires on the outside of his body needed to be replaced. It happens to him, too. There’s one key difference, though: several years ago, Abram managed to track down Kevin Kilgore, one of the researchers who developed the technology with Peckham in Cleveland. And Kilgore has been sending him wires over the years.
The situation mystifies and upsets Kilgore as much as anyone. When NeuroControl was in business, it supplied the Freehand to surgeons who installed it and served as the patients’ point of contact. From the perspective of patients like Mumford, the researchers who had originally invented the technology were not in the picture at all. When NeuroControl folded, nearly everything about it fell into a black hole. Not only did it fail to arrange technical support for its customers, but its website and phone number went out of service, leaving both the surgeons and the patients in the dark about what they might do next. Kilgore and Peckham say the company even refused to give them a list of patients who had gotten the implants. To this day the engineers say they don’t know exactly how many there were.
For Damion Cummins of Monroe, Louisiana, the company’s demise had a surreal aftermath. He had gotten the Freehand after being paralyzed in a high school football game. But it didn’t consistently work as well as he hoped, and he stopped using it after less than two years. Stopping was easy enough—he no longer asked someone to tape the awkward external wires to the device in his chest. But as the years went on, he wondered about that dormant electrical equipment, some of which you can feel right under his skin. “Is it going to disintegrate or break off?” he asked himself. “Should I worry about that?” He thought about going to see the surgeon in Shreveport who had implanted the Freehand, but the doctor had moved to California. Cummins says he spent a few years feeling uneasy about the electronics in his body before he finally tracked down the surgeon and called him. “Should I have it taken out?” Cummins asked. “No, as long as nothing’s bothering you,” the doctor said.
It’s painful for Kilgore to hear about the isolation that Cummins felt. About five years ago Kilgore got a $75,000 grant from Paralyzed Veterans of America, a nonprofit group, to follow patients with electrical-stimulation implants over an extended period. He spent much of the money buying up one of the few chunks of NeuroControl that hadn’t completely vanished: its inventory of wires, stimulator coils, controllers, batteries, and other Freehand parts, which another Ohio company had bought and was keeping in a warehouse. With that stockpile, Kilgore reached out to the Freehand patients he and his colleagues did know of—a few dozen people in Ohio—and set up an online users’ group in hopes of finding more.
In 2009, Kilgore and other researchers tracked down 65 Freehand recipients and determined that more than half were still using the device. Today he estimates that he has enough parts to keep such patients going for a few more years. But eventually, he says, “the ultimate fix” is for the patients to get something better. Nearly 30 years after the birth of the Freehand, the Case Western team has improved the technology significantly. Among other things, they have made the control unit small enough to be implanted in the body, eliminating the need for external wires that can snag and break. The device can also do more than restore grasping ability. It can be networked, as they put it, to send electrical stimuli to many more muscles—providing upper-body support, for example, or bowel and bladder control. The researchers have gotten some paralyzed people to stand and take halting steps with the help of a walker.
The essential economic dilemma remains, though: without a company to market this technology widely, the pool of potential recipients is limited to people who live in or can afford to travel to Cleveland. And if it’s not a commercial product, insurance companies won’t cover the cost of the device. That means the researchers have to rely on grant money to get these technologies into patients. “I can do five implants a year on grants,” Kilgore says. “But I get 100 phone calls a year.”
Even hundreds of patients a year might not make for a big enough market to entice private investors. But Kilgore and Peckham think they may have figured out a solution.
Deepening the pool
They are convinced that avoiding a repeat of the NeuroControl fiasco with many future implantable technologies will require a nonprofit/for-profit partnership. They’ve formed the nonprofit: the Institute for Functional Restoration at Case Western. Its mission is to usher technologies through regulatory approval; after that it could market the devices itself or license them to for-profit companies. Ideally, if such a company failed, the nonprofit—funded mainly by a private foundation—could keep supporting patients.
The first technology the institute will handle will be the networked device that is the descendant of the original Freehand. The organization has grants to begin a clinical trial and even to develop a manufacturing facility for the devices. It also has a waiting list of potential patients. But it has yet to sign up any companies as for-profit partners—companies that, as Peckham puts it, are “not trying to meet some venture expectations of how fast you return their investment.”
In theory, there could be many potential partners. As it happens, the neurostimulation business is enjoying a renaissance, especially in Cleveland, given the abundance of technologies to license from Case Western, the Cleveland Clinic, and other centers there. Several of the companies are staffed with alumni from NeuroControl, including Thrope, who now heads NDI, a firm that invests in neurotechnologies. Thrope says partnering with a nonprofit would be attractive to companies that don’t want to bear the risks inherent in taking a new technology through years of testing and regulatory approval. If the nonprofit can handle that part and then turn things over to a for-profit company, Kilgore and Peckham’s model “has some worthiness to it,” he says.
But even with that risk removed, Thrope is quick to add, not a lot of companies are interested in selling products that only a small group of people can use. Instead, he says, he and other investors are eager to find opportunities to address what doctors call multiple “indications,” meaning they can treat more than one condition. He mentions Second Sight, a publicly traded maker of a $140,000 retinal implant that can restore sight to people with a hereditary form of blindness. The potential market is quite big—perhaps 1.5 million people worldwide and 100,000 in the United States—but even so, Second Sight is already testing ways to deepen the pool of patients by treating other forms of blindness. Thrope says his firm, which he founded in 2002, rarely jumps in to invest in a neurotechnology until it has been developed beyond its initial stage and can treat a second or third indication. It’s “reversing the formula we used in NeuroControl,” Thrope says. “We’ve tried to avoid breakthrough technologies if possible.”
Avoiding breakthroughs: that seems to go against our tendency to imagine that technology will fix so many broken things, our bodies included. But consider the perspective of Damion Cummins. He says he endured multiple surgeries to get the Freehand because anything that could improve his daily life was worth a shot. He accepted the idea that it might not work. But when I asked him if he would have gotten the implant if he had realized there was a chance NeuroControl could fold, he replied: “If I had known that, then I definitely would not have.”

Advertisement