
Rewriting Life
A Tale of Two Drugs
Today’s medicines can cost hundreds of thousands of dollars a year. The story of how two companies set prices for their costly new drugs suggests that the way we determine the value of such treatments will help decide the future of our health-care system.

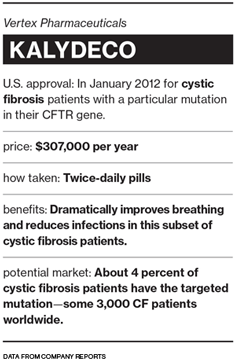
In January 2012, the U.S. Food and Drug Administration approved Kalydeco, the first drug to treat the underlying cause of cystic fibrosis, after just three months of review. It was one of the fastest approvals of a new medicine in the agency’s history. Vertex Pharmaceuticals, which discovered and developed the drug, priced Kalydeco at $294,000 a year, which made it one of the world’s most expensive medicines. The company also pledged to provide it free to any patient in the United States who is uninsured or whose insurance won’t cover it. Doctors and patients enthusiastically welcomed the drug because it offers life-saving health benefits and there is no other treatment. Insurers and governments readily paid the cost.
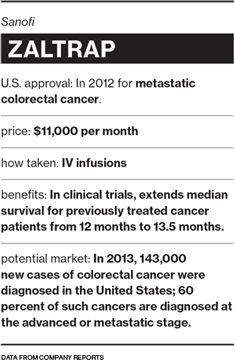
Several months later, Zaltrap was approved to treat colorectal cancer. The drug was discovered by Regeneron, an emerging biopharmaceutical company like Vertex, but sold by the French drug maker Sanofi. Though it worked no better in clinical trials than Roche’s cancer drug Avastin, which itself adds only 1.4 months to life expectancy for patients with advanced colorectal cancer, Sanofi priced Zaltrap at $11,000 a month, or twice Avastin’s price. Unexpectedly, there was resistance. Doctors at Memorial Sloan-Kettering in New York, one of the world’s leading cancer centers, decided Zaltrap wasn’t worth prescribing. They announced their decision—the first time prominent physicians anywhere had said “Enough” to the introduction of a high-priced cancer drug—on the op-ed page of the New York Times. Three weeks later Sanofi effectively dropped its price by half through rebates to doctors and hospitals. Even so, British health authorities said they would not pay for the treatment.
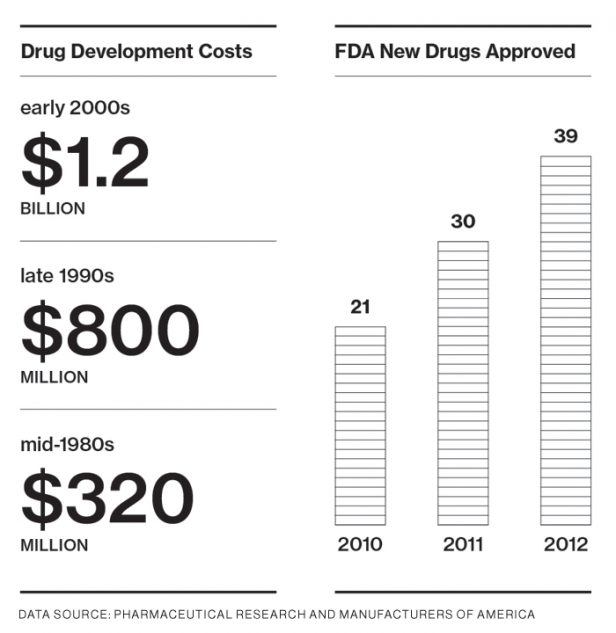
The FDA approved 39 new drugs in 2012, the most in a decade and a half—a sign that the pharmaceutical industry may be recovering from its long fallow period. Wall Street applauded the revival, especially because many drug companies are facing patent expiration for their top-selling products and could see dwindling revenues after years of lackluster research productivity. Most of the new drugs either treated rare diseases like cystic fibrosis or were marginal improvements over existing cancer drugs. All carried extremely high price tags.
But a closer look at the rollouts of Kalydeco and Zaltrap reveals startling differences in how companies value a drug and justify its price. It also provides a preview of a likely future in which extremely costly drugs are common.
Because of medical insurance, co-pay reductions, and expanded access programs for the uninsured, relatively few Americans pay more than a few thousand dollars per year for even the most expensive drugs. The primary customers in the United States are not patients or even individual physicians, although physicians can drive demand for a drug; rather, the customers are the government (through Medicare and Medicaid) and private insurance companies. And since the insurer or government is picking up the check, companies can and do set prices that few individuals could pay. In the jargon of economics, the demand for therapeutic drugs is “price inelastic”: increasing the price doesn’t reduce how much the drugs are used. Prices are set and raised according to what the market will bear, and the parties who actually pay the drug companies will meet whatever price is charged for an effective drug to which there is no alternative. And so in determining the price for a drug, companies ask themselves questions that have next to nothing to do with the drugs’ costs. “It is not a science,” the veteran drug maker and former Genzyme CEO Henri Termeer told me. “It is a feel.”
There are inherent problems with a system where the government is one of the biggest payers, and where doctors, hospitals, insurers, pharmacy benefit managers, drug companies, and investors all expect to profit handsomely from treating sick people, no matter how little real value they add to patients’ lives or to society. Drug companies insist that they need to make billions of dollars on their medicines because their failure rate is so high and because they need to convince investors it is wise to sink money into research. That’s true, but it’s also true that the United States, with less than 5 percent of the world’s population, buys more than 50 percent of its prescription drugs. And it buys them at prices designed to subsidize the rest of the industrial world, where the same drugs cost much less, although most poor governments can’t afford them at even those lower prices.
Still, we have to ask: When is the high price of a drug acceptable? Perhaps it is one thing when Vertex charges $841 for two pills a day—every day of a patient’s life—for medicine that will save that life, and quite another when Sanofi offers a cancer drug that is twice as expensive as its alternative but offers no obvious advantages.
Sticker Shock
A cruel and wasting disease, cystic fibrosis is the most common fatal inherited illness among people of European descent, affecting 70,000 patients worldwide, mostly in North America and Western Europe. The disease results from a malfunctioning protein embedded in the membranes of the densely packed epithelial cells that line the body’s cavities and surfaces. The CFTR protein is an ion channel, allowing chloride ions and water in and out of cells. When it is misshapen, the ions are blocked, causing the tissues to become congested with thick mucus secretions. This blocks up the pancreas, the gastrointestinal tract, and, often lethally, the lungs and airways. The mechanism underlying CF is both breathtakingly simple (a single broken protein) and harrowingly diverse (there are 1,900 known mutations of the disease-causing gene).
A generation ago, people with cystic fibrosis seldom survived their teens, and there were few effective ways to alleviate the devastating symptoms. (Even today, many patients have to have their chests routinely “pounded” to loosen the mucus.) But the Cystic Fibrosis Foundation (CFF), a hard-charging pioneer among disease charities actively seeking cures, did much to change what it means to live with the disease. By raising and investing more than $600 million to support the development of life-sustaining therapies, the foundation has helped develop treatments that have nearly tripled life expectancy by relieving symptoms. After pressing for years to find a partner willing to look for drugs that address the genetic problem at the disease’s core, the foundation invested in 2000 in Aurora Biosciences of San Diego, which was acquired by Vertex the following year. The CFF eventually committed more than $100 million toward the company’s discovery and early development efforts.
Kalydeco is one of two types of molecules Vertex is developing for cystic fibrosis, and the decision to move first with this one raised difficult questions inside and outside the company. The great majority of people with the disease have what are called folding mutations; their CFTR, malformed, never gets to the cell surface. Kalydeco, however, fixes only a so-called gating mutation—there’s sufficient protein at the membrane, but the channels don’t stay open long enough to allow the ions through. It’s designed to treat just 4 percent of CF patients, about 3,000 people worldwide; Kalydeco is currently approved only for adults and children six and older, lowering the eligible total to 2,400 people. Advancing a drug that doesn’t help most CF patients put both Vertex and the CFF (which would receive significant royalties) in the awkward position of targeting a tiny population while the vast majority of sufferers waited for the company to introduce a drug that could correct for folding mutations. But given the state of the science, Kalydeco seemed to offer the quickest route to saving at least some patients.
Vertex knew it could set a high price for Kalydeco because clinical trials showed striking results. Patients receiving the drug recorded a 17 percent improvement in breathing, when even 5 percent can mean a substantial gain in quality and quantity of life. No other drug had ever come close to providing such a benefit. The drug left patients feeling dramatically better and harboring new hope for the future, since declining breathing and more infections are the surest signs that a CF patient is nearing the end.
The company also knew it must convince insurers and doctors that the drug was worth the cost. “We talk about the value of Kalydeco in four ways,” Vertex’s chief pharmacoeconomist, Kyle Hvidsten, explains: severity of disease, effectiveness, safety, and “estimated magnitude of benefit.” Vertex reviewed actuarial studies and models of how much Kalydeco might be worth, given that people with cystic fibrosis take up to a dozen other medications daily, require frequent hospitalization, deteriorate substantially as they get older, and sometimes can be rescued only with a double lung transplant. The company projected that by significantly increasing a patient’s breathing measurements and improving other risk factors like absorption of calories, Kalydeco “may double the residual life for appropriate CF patients.” Vertex included the data in a report, more than 200 pages long, that it used to respond to questions from pulmonologists and other experts who advise insurers on what they should pay.
At launch, Kalydeco cost more than all but a handful of other medicines—close to $300,000 a year. But because it was highly effective and had no competitors, and because the budget impact was low given the alternatives, private and government insurers in the United States reimbursed for it, while worldwide payers started to take a closer look at its benefits. And yet the price alarmed many people. Vertex’s value equation—which hadn’t, after all, grappled with the larger societal issues of who pays and who benefits—failed to persuade some experts. David Orenstein, co-director of the Palumbo Cystic Fibrosis Center and chair of the ethics committee at Children’s Hospital of Pittsburgh, welcomed Kalydeco’s approval, but he felt strongly that the price represented a major escalation in the problem of soaring drug costs.
“I think everybody just went, ‘Whoa, that doesn’t seem right,’” Orenstein told me. He didn’t think there was anything he or anyone else could do to change the price, but he believed he and his colleagues couldn’t “sit back.” The center had participated in human trials of the drug. Considering the cost of other CF treatments, he and his colleagues had guessed that the price might exceed $100,000. Now the shock of Vertex’s actual price jolted them to act. He and four colleagues wrote a letter stating their concerns and recruited two dozen cosigners from across the country. In July, Orenstein sent the letter to Vertex CEO Jeffrey Leiden. After praising Kalydeco and saluting the company’s ongoing efforts against CF, the authors voiced several objections:
We also write with feelings of dismay and disappointment that the triumph and honor that should be yours is diminished by the unconscionable price assigned to Kalydeco. We are aware of the financial complexities of the huge expenses for R&D with respect to the small number of patients or the market system that enables these advances to become a reality. Yet—notwithstanding all your patient support programs—it is at best unseemly for Vertex to charge our patients’ insurance plans (including strapped state medical assistance programs) $294,000 annually for two pills a day (a ten-fold increase in a typical patient’s total drug costs). This action could appear to be leveraging pain and suffering into huge financial gain for speculators … We write with the sincere hope that you will find a way to reflect the humility, generosity of spirit, and consideration of the people—not millionaires—who will benefit from these drugs. Otherwise, we fear that they, and our medical system, face ruin by costs driven by “what the market will bear.”
Leiden was eager to defend his company and its drug. He wrote Orenstein back, saying he’d be happy to fly to Pittsburgh to talk. Orenstein, not knowing what to make of Leiden’s offer, discussed it with his colleagues, who together decided that “we didn’t want to put ourselves forward as the moral squad.” They proposed instead that a somewhat larger group sit down with Leiden and others from Vertex at the annual North American Cystic Fibrosis meeting in Orlando in October 2012.
At What Price?
Leiden declined to speak for this article, but no one disputes what happened next. “Jeff did most of the talking,” Orenstein said. “He was very charming and seemed very open. He wanted this to be the first of many meetings. We felt a little uneasy representing the entire CF community, but he said he wanted our input, wanted to work together. The reason we wrote the letter was the price, but when we tried to get back to that he was less convincing.”
Paul Quinton, a prominent researcher at the University of California, San Diego, whose early work contributed to Vertex’s approach and who himself has CF, recalls Leiden saying that the company was relying on the income from Kalydeco to finance its goal of curing cystic fibrosis by 2020. No one questioned Vertex’s commitment: the company had one “corrector” for the most common folding mutations in advanced human testing, and excitement was soaring about the prospects for combination therapy with Kalydeco—one or two drugs to propel the protein to the cell surface, another to open the channel. But Quinton was troubled by Leiden’s logic. “I came away relatively uncomfortable,” he says. “The Vertex message was that they needed our support, and if they don’t have it they’re at risk that their share price will come down and they’ll get bought out. If we’re not all together on this, we’ll lose 2020.”
Leiden showed he was serious about working with Orenstein and his group. “Jeff wrote to us: ‘What are we gonna do next?’” Orenstein says. “We had another conversation with him. He said, ‘Why don’t you come out to our San Diego site so we can have a meeting? A few dozen people.’ That wasn’t something we wanted to do, be wined and dined. I was sure that our socks would be blown off by what they’re doing there. But spending all these bucks to fly us out there to win us over to their side was a little disturbing. It’s great what they’re doing both medically and individually for patients, but we think that dodges the pricing question.”
Outside the United States, what the market will bear is decided by government regulators, and in that environment Vertex found it harder to help make sure that all patients would have access to Kalydeco. As the company negotiated with foreign authorities, news reports—first in England, Ireland, and Scotland, then in Australia, New Zealand, and Canada—focused on patients, usually children, who would benefit from the drug but couldn’t get it because their families couldn’t afford it. Negotiating on price, the company moved aggressively to give patients in the U.K. and Ireland access to the drug, a company spokeswoman told me in July. In Canada, however, patients are still waiting.
When Orenstein first wrote Leiden about Kalydeco, he worried what would happen if Leiden said to him, “Okay, you’ve convinced me. What would be a better price?” Orenstein concedes he doesn’t know, and that the Kalydeco story—a triumph medically and a home run financially, with Vertex sales beating expectations and the CFF recently selling a portion of its royalties for a reported $150 million that it has pledged to fund additional research—is probably the wrong place to start building an argument against immorality, waste, greed, and excess in the pharmaceutical industry. Kalydeco is different from other drugs in two important ways, he says: “There’s no comparable drug. And this truly is a breakthrough, offering much more value than what’s out there. If their only concern is what the market will bear, they’re going to get that price.”
Indeed, earlier this year Vertex raised the price of Kalydeco to $307,000. Orenstein’s group and Leiden continue to seek ways to work together, though Quinton and others remain bitterly disappointed. “I don’t want to hold myself up as a self-righteous SOB, but this really disturbs me,” Quinton told me. Orenstein, on the other hand, appears more understanding of the tough choices facing companies like Vertex. In view of the patients transformed by Kalydeco, he concedes, “This may be the best outcome: what we have.”
Cost Matters
In May 1998, the New York Times published a front-page story by Gina Kolata extolling two new chemical compounds “that can eradicate any type of cancer, with no obvious side effects and no drug resistance—in mice.” Kolata reported on the findings of Judah Folkman, of Boston Children’s Hospital, whose 30 years of work led to the discovery of angiostatin and endostatin. Used in combination, the compounds cut off the supply of blood to tumors, starving them while leaving the tissue around them untouched. Nobel laureate James Watson, co-discoverer of the DNA double helix, told Kolata, “Judah is going to cure cancer in two years.”
Throughout the pharmaceutical industry, companies scrambled to start their own programs targeting the mechanism Folkman named angiogenesis. The first great winner of the angiogenesis sweepstakes was a bioengineered antibody that blocks the activity of a molecule called VEGF, which stimulates the growth of new blood vessels. Roche’s Avastin was approved in 2004 for advanced colorectal cancer and is also used, in low doses, for treating macular degeneration, a common cause of blindness characterized by abnormal growth of blood vessels in the retina. Meanwhile, Regeneron, a company with a proprietary technology for “trapping” molecular targets, developed ziv-aflibercept, or VEGF Trap, which performed similarly. In the excitement over Avastin, Regeneron partnered with the French drug maker Aventis, which later merged with Sanofi. That company introduced Zaltrap in August 2012.
During those intervening years, cancer wasn’t cured, and a new economic order emerged in which many doctors, hospitals, and clinics actually make more money as prices for cancer drugs rise. This new order helps account for why Avastin, which it turns out seems unlikely to significantly improve the health of more than a relative handful of patients, had $6 billion in global sales in 2012. Avastin and Zaltrap must be administered intravenously in a medical setting. Cancer treatment centers and physician groups purchase drugs at a price set by the manufacturer and then seek reimbursement from payers at a higher price—a practice called “buy and bill.” The spread, or “cost recovery,” between the acquisition price and the reimbursement price drives revenues.
It’s not hard to guess where many hospitals and doctors stand on pricing. Of course they feel their patients’ suffering and financial hardships, but lower drug prices hurt business. Small, cash-strapped local practices, unable to maintain supplies of expensive drugs, have increasingly been squeezed out while major university hospitals and for-profit cancer networks compete for new territories, technologies, and patients. As a result, these advanced medical facilities tend to prosper and can offer some of the most sophisticated and effective treatment programs in the world. Offering the latest advances in treatment is good medicine, but it’s also a business imperative.
At Memorial Sloan-Kettering and other major cancer centers, the list of prescribed drugs is updated by a medical staff advisory group consisting of clinicians and pharmacists. The panel at Sloan-Kettering was unimpressed with the Zaltrap data, and after discussing the cost, it contacted Peter Bach, director of the hospital’s Center for Health Policy and Outcomes. Bach formerly served as senior advisor to the administrator of the Centers for Medicare and Medicaid Services, which oversees health care for 100 million people, and he writes frequently on reimbursement issues for the Journal of the American Medical Association and other publications.
“We went over all the [Zaltrap] data,” Bach told me. “We decided not to give the drug to patients, purely on the basis that it cost more without providing additional benefit. We appreciated that we were doing something that hasn’t been done, but we thought there was a point to be made.” Soon after, Bach and his coauthors, including the chief of the hospital’s gastrointestinal oncology service and the physician in chief, announced the hospital’s decision on the Times op-ed page under the headline “In Cancer Care, Cost Matters.”
Perverse Priorities
Sanofi reacted vigorously, determined to defend its pricing decision. But since Zaltrap doesn’t offer any documented advantages over Roche’s Avastin, it had to build its case on something other than value to patients.
The company dispatched executives to explain that Zaltrap’s price was consistent with that of other “second-line” drugs used to treat colorectal cancer as a last resort, after the standard of care has failed. In an interview with Paul Goldberg of The Cancer Letter, a publication about the business of cancer research and treatment, Paul Hawthorne, vice president and head of the oncology business unit at Sanofi U.S., and a colleague laid out the decision and the process that led to it.
“You look at a lot of things,” Hawthorne told Goldberg. “You look at the current marketplace; you look at how things are being used; you look at the number of agents that are valuable in second-line, including Erbitux and Vectibix; you look at the value that you are bringing into the marketplace; and you look to set a responsible price, which I think is what we looked to do when we launched Zaltrap.”
They had badly miscalculated. On November 8, three weeks after the Sloan-Kettering announcement, Sanofi said it would effectively cut the price of Zaltrap in half.
The company didn’t change the drug’s official price but offered rebates and other discounts of about 50 percent. Here in a nutshell were all the perverse priorities of “buy and bill.” Sanofi’s action was a giveback to doctors who prescribed Zaltrap. In other words, the decision wasn’t calculated to bring down costs for payers but to induce doctors and institutions to capitalize on the exceptional spread and order the drug now—while the offer lasted. “All of a sudden the doctors are getting a check from the government and from Sanofi,” Bach says.
Sanofi’s original pricing strategy and its subsequent physician-friendly price cut is a startling demonstration of how cost arrangements can distort treatment by encouraging doctors and hospitals to prescribe drugs offering no or limited clinical benefits for their patients. But the Sloan-Kettering pushback also shows how a single influential committee with strong institutional backing can make a significant difference. Like Vertex with Kalydeco, Sanofi encountered additional problems when it tried to launch Zaltrap in Europe. In June, the U.K.’s drug watchdog, the National Institute for Health Care and Excellence (NICE), turned the drug down for reimbursement. In its analysis, NICE estimated the cost per “quality adjusted life year,” or QALY—a measure of disease burden used to assess the value of a medical intervention in terms of impact on both quality and quantity of life. The per-patient cost to the National Health Service would be about $100,000, and the NHS already offered six other treatments for advanced colorectal cancer. “Although the independent committee considered [Zaltrap] to be a clinically effective treatment,” the advisory panel concluded, “it could not be considered a cost-effective use of NHS.”
Breaking Point?
Ultimately, what matters in pricing a drug is its value. Vertex succeeded in pricing Kalydeco because the medicine really works, because the company’s scientists knew the exact genetic profile of the people who would benefit, because they were able to show definitive clinical results in well-designed trials, and because the company ensured that the right patients got the drug and that access was no issue. The drug makes a true difference where nothing else does. Sanofi has failed—so far—with Zaltrap because it’s not yet known what the drug may do for individual patients, because the only way to find out who will benefit is through costly, inefficient trial and error, and because its value is at best uncertain and at worst no greater than that of a barely effective alternative at half the price.
If current research is successful, we’re likely to see more and more cancer drugs that are highly effective for a limited and defined group of patients, as Kalydeco is for a small subset of people with CF. That’s good news for those patients, but it will drive the costs of drugs even higher. William Oh, chief of the division of hematology and medical oncology at Mount Sinai Hospital in New York, suggests that the past few years in cancer research marked a turning point. He expects that as doctors learn more about the genetic make-up of patients and the specific mutations driving their disease, and as earlier detection becomes the norm, cancer treatments will become increasingly targeted, and they’ll be ever more effective for the appropriate patients.
“We’ve begun to expect that drugs should be developed specifically for this or that abnormality,” says Oh. “A decade ago that would have been unheard of—you either have a drug that treats all lung cancer, which is a very large population, or you don’t, and you just see if it works or not. But now we know that if you have that abnormality in your cancer, you have a very high response rate to that drug. The problem is in cancer we’re talking about lots of different diseases, with dozens and dozens, maybe hundreds, of different abnormalities that are driving these cancers. That makes the ability to develop drugs to target each subset very, very difficult and in some ways even more expensive.”
Figuring out which patients will benefit most from which combinations of drugs is the only thing, in the end, that could enable some kind of value-based pricing method to take hold in the U.S. There are a few early examples of progress toward this goal. For example, more than 60 percent of new drugs in the works at Roche are being developed along with gene-based diagnostic tests to identify the patients most likely to benefit. Such tests would optimize outcomes and costs, thus bringing greater rationality into the process of pricing new treatments. Oh says, “I think everyone realizes this is a huge priority: basically to figure out which patients are going to benefit from which drugs, both because of the costs of the treatments and because the diseases themselves are so heterogeneous.”
Though the advent of these more targeted, more effective drugs will introduce the prospect of ever-rising prices, highly effective and ultra-expensive so-called orphan drugs like Kalydeco may impose a stricter rubric for determining the price of all new medicines. Being able to more precisely identify the effects of new treatments and the patients who will benefit from them should finally allow companies to price these drugs on the basis of their true value. Whether the resulting prices are “worth it” will then be up to society to decide.
Barry Werth’s book The Billion-Dollar Molecule (1994) describes the early days of the startup Vertex. A sequel, looking at Vertex 20 years later, is called The Antidote and is due out in February.
Advertisement