Mapping how our neural circuits change under the influence of anesthesia could shed light on one of neuroscience’s most perplexing riddles: consciousness.
Going under: Emery Brown’s quest to understand how anesthesia affects the brain could provide crucial clues about what goes wrong in certain disorders.
Mapping how our neural circuits change under the influence of anesthesia could shed light on one of neuroscience’s most perplexing riddles: consciousness.
Going under: Emery Brown’s quest to understand how anesthesia affects the brain could provide crucial clues about what goes wrong in certain disorders.
A video screen shows a man in his late 60s lying awake on an operating table. Just outside the camera’s view, a doctor is moving his finger in front of the man’s face, instructing him to follow it back and forth with his eyes. Seconds later, after a dose of the powerful anesthetic drug propofol, his eyelids begin to droop. Then his pupils stop moving. Only the steady background beeping of the heart monitor serves as a reminder that the man isn’t dead. “He’s in a coma,” the doctor, Emery Brown, explains. “General anesthesia is a drug-induced reversible coma.”
As an anesthesiologist at Massachusetts General Hospital (MGH), Brown is constant witness to one of the most profound and mysterious feats of modern medicine. Every day, nearly 60,000 patients in the United States undergo general anesthesia, enabling them to survive even the grisliest operations unaware and free of pain.
But though doctors have been putting people under for more than 150 years, what happens in the brain during general anesthesia is a mystery. Scientists don’t know much about the extent to which these drugs tap into the same brain circuitry we use when we sleep, or how being anesthetized differs from other ways of losing consciousness, such as slipping into a coma following an injury. Are parts of the brain truly shutting off, or do they simply stop communicating with each other? How is being anesthetized different from a state of hypnosis or deep meditation? And what happens in the brain in the transition between consciousness and unconsciousness? “We know we can get you in and out of this safely,” Brown says, “but we still can’t quite tell you how it works.”
Brown, who is also a neuroscientist and professor at MIT, aims to transform anesthesia from a solely clinical tool into a powerful instrument for studying the most basic questions about the brain. Understanding what happens to the brain under anesthetic drugs, he believes, will help make anesthesia safer and more effective, with fewer side effects. It could also lead to novel treatments for coma and other brain conditions—and to insights into fundamental questions in neuroscience, including the nature of consciousness itself. “Anesthesiology is a form of neuroscience,” says George Mashour, an anesthesiologist and neuroscientist at the University of Michigan. “And what we do on a daily basis is modulate virtually every aspect of the nervous system.”
FROM CHATTER TO CHANT
Neuroscience has often benefited from natural experiments—patients who lose their ability to remember, produce language, or regulate their emotions after parts of their brains are damaged or have to be surgically removed. Anesthesiologists preside over an analogous experiment every day: they watch elements of consciousness disappear. Under general anesthesia, for instance, patients lose pain perception, awareness, memory, and the ability to move. An anesthesiologist can influence each of these changes in different ways by varying the dosages and types of drugs used.
“By taking away different functions that we associate with consciousness,” Brown says, “we might be able to start piecing together parts of the jigsaw puzzle.” Neuroscientists could begin to do for consciousness what they have done with memory and language.
Brown is part of a small but growing group of anesthesiology researchers who are using the electroencephalogram (EEG), a tool for monitoring the brain’s electrical activity, to systematically probe each aspect of anesthesia in humans and animals. EEG-based brain monitors are already a common sight in operating rooms; some anesthesiologists track the brain activity of their patients with commercially available monitors that use algorithms to transform EEG signals into crude indexes. (Others track only physical signs such as heart rate and blood oxygen levels.) But few of them, he says, spend time looking at the raw EEG data.
Brown, however, has a different perspective from most anesthesiologists; he’s also a statistician. After receiving both an MD and a PhD from Harvard in the late 1980s, he pursued the two paths separately, working in the operating rooms of MGH while heading a research laboratory focused on developing signal-processing algorithms to extract information from biological data.
Brown didn’t appreciate the neuroscience experiments taking place in front of him each day during surgery until one of his colleagues suggested doing a study on anesthetized patients. Watching the process unfold, “you start realizing that parts of the brain don’t shut down all at the same time,” he says. “There is a hierarchy, there is a gradation to it.”
The same is true when the drugs wear off. Typically, the most basic brain functions come back first—breathing returns, and then, as the areas of the brain stem controlling salivation and tear ducts revive, patients’ mouths fill with saliva and their eyes water. They swallow and cough as areas controlling sensation to the throat become active. Finally their eyes move, and then they respond to the outside world. Later the grogginess will lift and complex brain functions will resume. “When you pay attention and you watch those transitions, it’s just amazing,” Brown says. “We would truly be remiss if we didn’t then move forward and try to figure out what these states are, what’s actually happening in the brain, and then think of new ways to improve the anesthesia process.”
One of the things that struck Brown from watching his patients’ EEGs is how quickly and completely drugs like propofol can alter brain activity. As patients enter an anesthetized state, the normal pattern of low-intensity but high-frequency waves shifts to one of less frequent but more intense pulses—as if the constant chatter of the brain had given way to a chant. The location of activity shifts from the back of the brain to the front. Although it’s possible to take patients into such a deep state of unconsciousness that their EEG is essentially flat, in most cases bursts of EEG activity alternate with periods of relative inactivity that can last for minutes. The brain processes appear “highly organized,” he says. “There are very regular patterns in time, and very regular patterns in space.”
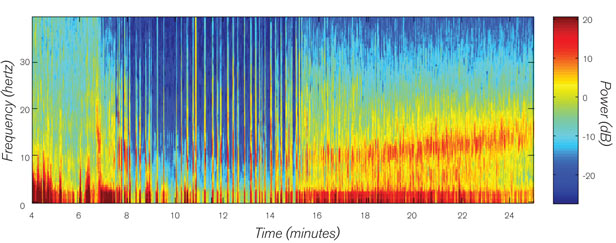
Charting the unconscious: This spectrogram shows EEG recordings from a patient undergoing general anesthesia. Two doses of the intravenous anesthetic propofol lead to bursts of activity (minute seven). Then an inhaled anesthetic, isoflurane, is added, and at minute 14, a characteristic pattern of slow-wave and alpha oscillations begins. Surgery ends at minute 16, and the isoflurane is switched off. The EEG gradually shifts to high-frequency, less intense oscillations.
Brown says that some drugs will decrease the frequency of brain waves seen in EEG readings, resulting in slow, regular oscillating waves across large areas of the brain. Other drugs cause certain areas to show fast, regular oscillations. Because anesthesiologists usually give a cocktail of drugs to each patient, these effects can happen simultaneously. The result, says Brown, is like a jammed signal: “Either way, [the different parts of the brain] can’t communicate.”
Over the past few years, other EEG studies have supported the idea that anesthesia doesn’t simply shut the brain down but, rather, interferes with its internal communication. Mashour’s research, for instance, has shown that feedback between the front and back of the brain is interrupted during general anesthesia, leading to a disconnect between different brain networks. That feedback is thought to be important for consciousness.
Similarly, Anthony Hudetz, an anesthesiologist at the Medical College of Wisconsin in Milwaukee, says that anesthesia doesn’t simply switch off the senses. Hudetz administers anesthesia to human volunteers at lower-than-clinical levels to observe their brains as they slip into unconsciousness. “What we find is that the anesthetized brain is still very reactive to stimuli,” he says; both EEG and functional magnetic resonance imaging (fMRI), an indirect method of measuring brain activity, show response to light and sounds. But somehow that sensory information is never processed and integrated into the type of activity necessary for conscious awareness.
Better understanding of these changes could point a way toward new treatments for brain injury and other disorders. The patterns of highly structured oscillations in patients given anesthetic drugs are similar to states seen in people who lose consciousness during epileptic seizures or who are in deep comas. And the semiconsciousness that results from low doses of the drugs resembles ordinary wakefulness or the early stages of falling asleep. But figuring out exactly how and why these patterns are related will take closer scrutiny.
MAPPING THE COMMUNICATION BREAKDOWN
In order to truly understand whether communication between different brain areas has broken down, scientists need a way to map the activity of these regions and the interactions between them in greater spatial detail. For that, they are turning to fMRI, which measures the changes in blood flow associated with neural activity (see “Raising Consciousness,” January/February 2007).
Working with bioengineer Patrick Purdon and other colleagues at MGH, Brown has developed a way to simultaneously take EEG recordings and perform fMRI scans on patients as they enter a deeply anesthetized state. Brain imaging in human subjects undergoing anesthesia is tricky because it requires anesthetizing people within a scanner and outside a normal operating room. Brown and his colleagues found a way to solve the technical and safety problems: they recruited volunteers who had already received tracheostomies, or surgical holes in the throat. That meant a tube could readily be used to restore their breathing in an emergency. In 2009, the researchers demonstrated that they could safely record both EEG and fMRI data on people under anesthesia; now they are working to correlate the imaging and EEG data with the observable changes seen as patients enter an anesthetized state.
Brown is also working with Purdon to study epilepsy patients who’ve had electrodes implanted into their brains for several days so that clinicians can record and locate seizures. When the patients undergo surgery to remove the brain areas identified as seizure sites, the electrodes record brain waves as anesthesia is administered. These electrodes collect data about a much smaller part of the brain than EEG or fMRI, but the resolution is much higher, allowing scientists to get a sense of what happens in the brain at the cellular level as the patient is anesthetized. Follow-up studies in animals could yield even greater detail by allowing the researchers to implant electrodes more extensively and in precise locations. The researchers will be able to document—from within the brain itself—how activity changes as the brain slips into and out of consciousness.
PIECING TOGETHER CONSCIOUSNESS
If you can systematically catalogue how the brain loses consciousness under the influence of anesthetic drugs, can you deduce what consciousness consists of?
Brown is quick to point out that he doesn’t explicitly study consciousness; it’s a messy problem, and many neuroscientists avoid the very word. His approach is to study what he calls altered states of arousal. These include anesthesia, sleep, coma, hypnosis, and meditation, as well as aspects of disorders like schizophrenia, epilepsy, and Parkinson’s disease. He believes that understanding how the brain functions when it deviates from its normal conscious state will inevitably shed light on what consciousness is.
Anesthesia studies have already cast doubt on one popular theory, which links consciousness to a particular type of brain wave with a frequency around 40 hertz. Mashour points out that research in anesthesia shows these waves can exist even when patients are unconscious. But the patterns that anesthesiologists see do support another theory: that consciousness emerges from the integration of information across large networks in the brain. Hudetz says that while different drugs have different chemical structures and different effects, such as blocking memory or sedating the brain, “if we give any of these drugs at a high enough dose, at some point they do remove consciousness. How do we get this common end point by such a variety of drugs working through different molecular mechanisms?” One explanation is that because consciousness arises from the complex interaction of many kinds of activity, it can be disrupted in many different ways.
Brown hopes the insights gleaned from this work can spill into other areas. Knowing more about how the brain functions under anesthesia could help researchers detect brain activity in people in vegetative states, revealing that they may perceive more than previously thought. The safer anesthetics that might emerge from the research could be useful in sleep medicine, and ways of reviving cognitive function in anesthetized patients might give rise to strategies for helping bring people out of comas. Ketamine, a commonly used anesthetic, has shown some promise as a treatment for depression; other anesthetic drugs could also prove to have effects that lend themselves to treating psychiatric illness. Studying the loss of consciousness in anesthesia will not just illuminate the nature of the conscious mind but bring these states of dampened or altered consciousness out of the shadows.
Courtney Humphries is a science writer and the author of Superdove: How the Pigeon Took Manhattan … and the World.