Record save: In the Boston Medical Center’s emergency department, Vera Sinue might have been subjected to a CT scan and other tests. But new electronic medical links with her community health center reassured doctors that her mysterious vomiting was not an acute issue.
Record save: In the Boston Medical Center’s emergency department, Vera Sinue might have been subjected to a CT scan and other tests. But new electronic medical links with her community health center reassured doctors that her mysterious vomiting was not an acute issue.
A crow flying from Vera Sinue’s apartment in Boston’s Roxbury neighborhood to her job as an insurance representative near the Charles River in Brighton would skirt the edge of the Longwood Medical Area, a district of medical institutions including Brigham and Women’s Hospital, Beth Israel Deaconess Medical Center, Children’s Hospital, the Dana-Farber Cancer Institute, and Harvard Medical School. These institutions are among the nation’s most respected. They supplied some of the experts now leading the Obama administration’s effort to reform the nation’s health-care system.
Yet it’s lucky for Sinue that when she began vomiting uncontrollably one day last August, she didn’t end up at any of the Longwood hospitals. Sinue, who is 35, gets her routine medical care at the Codman Square Health Center, in the heart of the low-income neighborhood of Dorchester. Her Codman Square records would not have been accessible to any of the Longwood emergency departments. While Boston’s medical institutions generally lead the nation in using advanced information technology for their own networks of physicians and satellite health centers (and the Longwood hospitals were early adopters), the networks don’t connect with one another to share data about patients’ medical histories and needs.
As it happened, Sinue went to Boston Medical Center, in the city’s South End, just a few weeks after Codman’s records became part of a network linking BMC with 10 community health centers. BMC, the teaching affiliate of the Boston University School of Medicine, runs New England’s largest trauma center and busiest free-care service. But it’s the links with the neighborhood health centers that are most remarkable. The health centers aren’t owned by BMC, so there were plenty of institutional barriers to their sharing patient data. And what this group of institutions has started doing to break down those barriers is an example of what the entire U.S. health-care system needs to do to make the best use of information technology. “In terms of a hospital taking the initiative to do what they have done–link together, using national standards, a set of individual physician-based medical records–it’s not all that common,” says John Halamka, CIO of Harvard Medical School and Beth Israel Deaconess Medical Center, who serves on regional and national bodies advancing health IT. “BMC is a leader in health-care information exchange.” The effort is especially significant because BMC serves so many low-income patients–who suffer disproportionately from chronic diseases and often have fragmented histories of care, making it all the more important for information to be shared among care providers.
Inside the BMC emergency room, Sinue’s vomiting did not stop. The attending physician, Aneesh Narang, was understandably worried. He asked if this had happened before; she muttered that it had happened only in childhood. A sudden and acute bout of vomiting might indicate appendicitis or ischemic bowel disease (the death of intestinal tissue), either of which would require speedy surgery. In the absence of more information, most emergency-room doctors would order a CT scan (at least $2,100), and possibly an abdominal ultrasound (another $500), to see what was going on. But Narang called up the electronic records from Codman and found lab data and physicians’ notes that spelled out her allergies, medications, and history of medical problems.
These records were certainly not cutting-edge medical IT–no genomic data, not even any images. But they would make a big difference. Narang quickly saw that Sinue hadn’t told the full story. In fact, vomiting was a chronic issue; it topped her list of medical problems. At one point she’d even had an endoscopic procedure to examine her digestive tract for signs of ulcers or other abnormalities. It’s not clear why Sinue hadn’t disclosed this information. (She later told me she might have forgotten.) Whether caused by stress, cultural differences, or language barriers, such miscommunication “is not really that surprising–we get it all the time,” says Andrew Ulrich, an emergency room physician who is also vice-chair of BMC’s emergency department. “You’d be amazed what people don’t remember. But this reassured us that this was not an acute problem.” Doctors knew they could skip the CT scan and the ultrasound, thus saving time and money–and sparing Sinue a dose of radiation from the CT test. She was treated with antinausea medication and intravenous fluids. Once the crisis passed, a talk with a physician revealed that Sinue was distraught over a personal issue. When the subject came up, she was overcome with nausea. She got a referral for what she probably needed most: counseling.
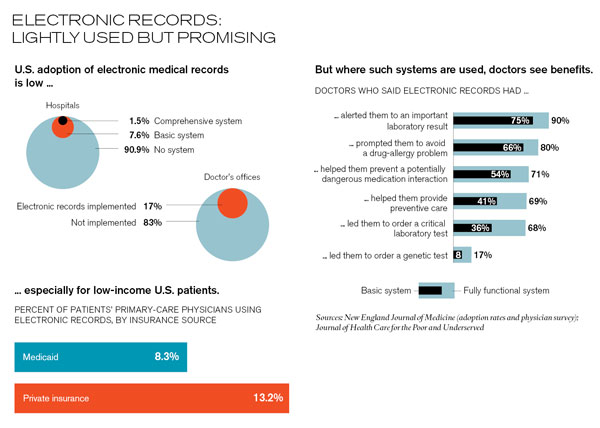
“Working in the Dark” Information technology–used properly and broadly–could help remake the U.S. health-care system. In 2006, the National Academies’ Institute of Medicine (IOM) called for a nationwide health-IT system to help prevent the drug errors that it said injure 1.5 million Americans every year. Electronic prescriptions, the organization argued, could eliminate problems caused by hard-to-read handwriting, and they could be incorporated into systems that would automatically catch physicians’ mistakes. The IOM had previously called for “electronic databases and interfaces” in a 1999 report finding that 44,000 to 98,000 Americans die annually from medical errors of all kinds. Using such technology, it found, could not only prevent fatal mistakes but also ensure that patients aren’t subjected to redundant tests, that they get cancer screenings in time, and that they manage chronic diseases more effectively. Yet progress has been painfully slow: though the number of physicians using electronic records has inched up over the past decade, 83 percent of them still use paper records today.
Besides improving or even saving patients’ lives, electronic records can potentially save money by reducing hospitalizations and eliminating unnecessary procedures, as they did for Sinue. In 2005, a think tank run by Partners HealthCare, the organization formed by Massachusetts General and Brigham and Women’s Hospitals (whose own network of hospitals and physicians uses some of the most advanced electronic-records applications in the nation), estimated that introducing this technology would save $78 billion nationwide.Though subsequent analyses have questioned that figure, nobody disagrees that the $2.3 trillion annual U.S. health-care bill includes staggering levels of waste. “If you ask how much in total medical spending there is in the country that doesn’t need to happen–providing absolutely no clinical benefit–the answer is probably about $700 billion a year,” says David Cutler, an economist at Harvard University and a former health-care advisor to President Obama. “Health-care IT is a fundamental part of getting rid of that. It is not the only important thing. But without information, you’ll never get rid of it.”
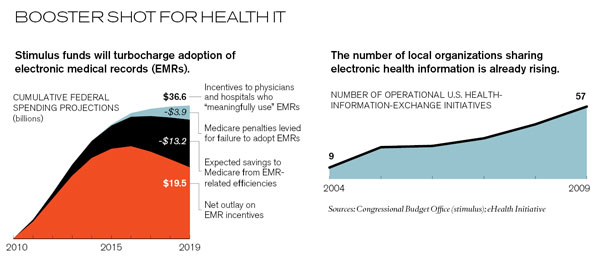
To promote effective use of such technology, Congress included huge incentives for health-IT purchases in the stimulus legislation passed earlier this year (see “Can Technology Save the Economy?” May/June 2009). Physicians and hospitals can collect cash–as much as $44,000 over five years for individual doctors, and millions of dollars for hospitals–if they document not only the adoption of electronic records but the “meaningful use” of that technology before 2012. “Meaningful use” is now being defined in detail by the Office of the National Coördinator for Health IT, led by David Blumenthal, a physician and former director of Partners HealthCare’s Institute for Health Policy (see Q&A). Doctors who don’t meet that standard before 2015 will face financial penalties: 1 percent taken from their Medicare fees in the first year, 2 percent in the second, and 3 percent in the third and subsequent years.
The ultimate goal: a privacy-protected Nationwide Health Information Network that would allow medical institutions across the country to exchange patient records. Hardly any of them coöperate in this way today; sharing electronic records between hospitals is a huge step beyond using them within hospitals. While a few robust regional networks have been running for years, they remain geographically limited. “As with electronic medical records, there are a few showcase places, and then there’s the whole rest of the world,” says Bonnie Kaplan, a lecturer in medical informatics at the Yale School of Medicine.
The public-health advantages of an integrated network could be tremendous: huge sets of regional and national data could be analyzed to help researchers to discern optimal treatment strategies, unearth dangerous drug side effects, and give early warning of epidemics and other large-scale problems. But lower-income patients might benefit more directly than any other group. They are more likely to have bounced around among various providers; they suffer disproportionately from chronic health problems such as diabetes, heart disease, and asthma; and they often end up getting primary care at emergency rooms. “Our patients, probably more than other patients, are not as able to advocate for themselves,” says Meg Aranow, the vice president and CIO of BMC. “They may have language issues. And we have cultural barriers, such that people are more or less comfortable talking to another gender or someone who is perceived to be of a different class. There are a ton of communication issues that burden our practice.” Even when such issues don’t arise, doctors or nurses often need records from other hospitals in order to give patients proper care. And today that generally means phoning records clerks and waiting for faxes to come through–a process that can take hours or days.
Nobody understands that problem better than Robert Gamble, a nurse practitioner with Health Care for the Homeless, one of the health centers now linked with BMC. His clients shuttle between shelters, transitional lodging at motels, and the streets. Gamble recalls a 28-year-old woman from Worcester, MA, obese and suffering from high blood pressure, who had been assigned temporary housing with her two-year-old son at a motel in Marshfield, 50 kilometers south of Boston. Gamble was traveling back and forth to see her, and trying to arrange medications for her–and immunizations for her son–through phone calls to her doctor in Worcester, 120 kilometers from the motel. “I’m used to working in the dark, just working from the issues that are presented in front of me,” he says. “It will be great to get more history, medication lists, and other background stuff.”
Long Slog It’s easy to understand why BMC wanted better connections with the community health centers, many of which serve poor and minority neighborhoods. Their patients often come to BMC for specialist visits or emergencies. But the hospital couldn’t build those connections until the smaller institutions computerized their records, and community health centers–which number about 1,200 in the United States–are particularly hard-pressed to invest in IT on their own, says Robert Miller, a health economist at the University of California, San Francisco. The Boston project, which originally targeted 15 health centers serving 206,000 patients, became possible only when an anonymous donor contributed $5.5 million in 2001.
The first three years were consumed by the effort to set up electronic records at the health centers and persuade staff to use them. “For a long time during the transition, the doctors at the health centers refused to let go of the paper record,” says Francis Doyle, executive director of Boston HealthNet, which runs the network. Once that hurdle was overcome, the first links were forged. Beginning in 2005, BMC doctors were able to log in and look up records in the databases of the individual health centers, though a separate password and user ID was still needed for each one. But the doctors and nurses at the health centers came to realize that these new links were of limited use unless all the centers and BMC networked their data to create a single patient record available to any clinician anywhere in the network. It would take $1.25 million in two grants from the U.S. Health Resources and Services Administration to create this truly integrated network–one that so far covers 10 health centers, not all 15 originally envisioned. (The other five will be added in the next year or two.)
To create a single, searchable system, BMC and the health centers needed to reliably match records for the patients in their respective databases. They did it with software from GE, one of several major health-IT vendors. The technology looks at birth dates, addresses, race, and other identifiers to distinguish patients with similar names and, conversely, to determine when records containing different addresses or differently spelled names actually refer to the same person. It creates a master index, but the actual patient data stays at the individual health centers. When a doctor logs in at BMC, the software pulls out the latest information from all sources. And a doctor needs to remember only one user ID and password.
The BMC network went live just this summer, so the hospital has not yet formally analyzed its impact. But anecdotes like the one about Vera Sinue have been trickling in. And after just two weeks, Dan Newman, BMC’s chief medical-information officer, stumbled across one of the system’s ancillary benefits. Newman had been treating a man in his 60s for chronic back pain. “I had had problems with this patient in the past,” he says. “He would show up every single month for his medication but wouldn’t go for any tests to work up the cause of his pain.” Sure enough, the system showed that the patient had visited several of the health centers: he was doctor-shopping to obtain prescriptions for painkillers. “They had Percocet on the medication list and were writing him for other drugs, too,” Newman says. He adds that the system has unmasked other patients doing the same thing. And data mining from eight of the connected health centers has already begun in an effort to improve patient care. A particular focus is on the chronic health problems afflicting the network’s patients. (To pick just one of many sad national statistics, African-American diabetics are 2.3 times as likely as white diabetics to suffer preventable complications that require amputation of a foot.) The eight health centers serve more than 70,000 adult patients and have begun tracking seven indicators of diabetes or heart disease–which affect more than 5,000 of them–while working on outreach strategies to help them manage their health. (More than half the patients in the network receive care at more than one of its facilities, so sharing the data is crucial.) The neighborhood health centers have also overhauled their notoriously inefficient process for managing referrals to BMC specialists. Previously, this process relied on the patients themselves, with uneven results. “We’d end up with patients sitting in the cardiologist’s office, and the cardiologist would ask, ‘Why are you here?’ and the patient would respond, ‘I have no idea,’” Newman says. “Some of them would say, ‘I don’t even know what my doctor’s name is.’” Now the specialists can call up the complete record. And with fewer repeated appointments, everybody is wasting less time.
Despite all this, a visit to BMC’s emergency room provides a reminder that electronic records, even those shared within an innovative hospital network, are of limited use unless the data is shared more widely across the health-care system. On the August day when Sinue came to BMC, only 164 of the 366 patients seen in its emergency room had previously visited that hospital or any of the 10 health centers. The rest had no records in the system: 77 said they had primary-care physicians outside the network, and 125 said they had no such provider at all. This latter group included Joycelyn Jobson, a 60-year-old woman who arrived complaining of pain in the left side of her abdomen. The doctors performed an electrocardiogram (EKG) and noted a slight abnormality in her heart rhythm. This was a red flag: it could have meant she was in the early stages of a heart attack. Or it could have been nothing–perhaps the vestiges of a cardiac event years earlier.
I went up to Jobson’s room. There, a resident, Jessica Eng, was trying to tease out more information.
“What’s wrong?” Eng wanted to know.
“This pain … bad feeling,” Jobson replied. “Won’t leave me alone.”
“How long?”
“Long time. Long time now.”
“What kind of treatment have you had for this?”
“Nothing.”
“Have they looked at it with scans or ultrasound?”
“Yes.”
“Have they ever had a camera inside?”
“No.”
It wasn’t clear whether real communication was actually happening, or whether Jobson even had an emergency; at one point, she told me she’d had the pain for 20 years. Doctors were hopeful when she said she’d previously been to the Codman Square Health Center. (She lives in Jamaica, where she and her husband raise yams and pigs on a small farm, but regularly visits her son and grandchildren in Boston’s Mattapan neighborhood.) Yet the database revealed no hits. And so an expensive medical odyssey began. She was admitted for observation and hooked up to machines that monitored her vital signs. Nurses checked blood pressure in both arms; a difference was noted. This can be harmless, or it can signify a life-threatening tear in the thoracic aorta. So the nurses wheeled Jobson in for a CT scan. No tear was found. But a radiologist examining the scan saw nodules in Jobson’s lungs. Though the nodules probably indicated infection rather than cancer, the discovery meant ordering another CT scan in three to six months to rule out a malignancy.
Data doctor: Andrew Ulrich, an emergency physician at Boston Medical Center, says miscommunication between doctors and patients is commonplace, and patients often don’t remember what medications they’re on. BMC clinicians can now consult detailed patient records linked to primary-care physicians at Boston-area community health centers. Such links can help resolve medical mysteries.
Plausibly, all of this could have been avoided if the doctors been able to find an earlier EKG showing that her cardiac abnormality was preëxisting. In the end, the doctors found nothing wrong. Three days later, Jobson was discharged. Her care probably cost something in the neighborhood of $15,000–surely a piece of the $700 billion in spending that the economist David Cutler was talking about. And doctors at BMC say the story is typical of patients for whom no records can be found. Vague complaints result in a fusillade of defensive and probably needless tests and treatments–a situation that is unlikely to change unless doctors and hospitals all around the country can share and analyze data electronically.
Balkanized Caregiving What will it take to stitch together all the health-care providers in greater Boston, let alone the entire United States? Linking disparate facilities is technically possible now, but the fact that it took BMC eight years just to make connections with 10 health centers shows how hard the process can be. Hospitals are businesses, after all, and don’t want to lose patients to competitors. Nor do they want to violate patient confidentiality, a risk that can increase as information is shared beyond a hospital’s walls. “What’s in it for the hospital to give up their data? What is the incentive?” says Larry Nathanson, director of emergency-medicine informatics at Beth Israel Deaconess Medical Center in Boston. “Right now, under the current model, there is a lot of risk involved if you are going to share your data. There is considerable risk, and there is little benefit. Except maybe a ‘herd benefit’–if you do it for me, I do it for you.” Beth Israel uses software developed by Nathanson to manage care in its emergency department, but the technology can’t access records at other hospitals in the area.
Massachusetts health-care executives have long discussed wider information sharing among clinical facilities, and they’ve even hammered out the technical prerequisites. But in Boston as elsewhere, medical institutions are still inclined to spend their IT budgets on their individual needs, concedes John Glaser, vice president and CIO of Partners HealthCare. (Glaser is now on loan four days a week to the Office of the National Coördinator of Health IT, where he is a senior advisor to David Blumenthal.) “From a research perspective, there is a lot of collaboration,” he says. “But a patient who moves from BMC to Brigham–does the data move with them? No. That is typical across the country. If you sit at a board meeting, whether at Brigham or Beth Israel Deaconess or BMC, and say, ‘All right, we have $10 million in capital funds and $40 million worth of requests,’ and one is to improve an IT system for nursing care, and another is to connect electronically with the Lahey Clinic, the one for the nurses is going to win every day.”
That should start to change as states begin receiving their share of the $564 million that Blumenthal has designated for jump-starting statewide and regional health-information networks. And the forthcoming “meaningful use” definitions are likely to include additional incentives for networking at the state and, eventually, national levels. Executives from most hospitals in eastern Massachusetts plan to start sharing discharge summaries (as patient records of hospital stays are called), something a few hospitals are already doing. And several pilot projects for data exchange are under way.
A national network of electronic medical records would not just promote greater efficiency and more consistent patient care; it could also give rise to unexpected insights. Consider the case of the onetime blockbuster anti-inflammatory drug Vioxx. It was a 2004 analysis of the electronic medical records of 1.4 million patients in the Kaiser Permanente health-maintenance organization that showed that users of Vioxx–on the market since 1999–were twice as likely to suffer heart attacks or strokes as people who took a rival drug, Celebrex. Later, Glaser says, Partners HealthCare looked at its own network data and found a similar pattern. “When you look at this data, your reaction is ‘Holy shit, we could have seen this in 2001!’” he says. “You can see the signal. The key question is: if we look at more and more of this data, can you see these kinds of signals much earlier?”
TB-free: Colleen Clougherty needed a medical checkup in the Boston Medical Center emergency department before entering a detox facility. An electronic record made reference to a positive tuberculosis test 14 years ago but didn’t say whether she was now TB-free. Doctors were poised to order a chest x-ray until a nurse made telephone calls to confirm that she was healthy. Sharing electronic records more widely among providers could spare patients from needless tests and radiation–and save costs.
But those benefits are abstractions in relation to clinicians’ daily struggle to make sense of isolated scraps of data on individual patients. Consider the hot August night when it fell to Dona Petrozzi, a psychiatric nurse in BMC’s emergency department, to line up the proper care for a Dorchester narcotics addict named Colleen Clougherty, who’d called for an ambulance after suffering from hallucinations. Clougherty wound up in a special guarded wing reserved for psychiatric emergencies. Her room had no furnishings other than an examining table bolted to the floor. Clougherty sat on its edge, clutching a blue stuffed bunny she’d brought. Gaunt, with slicked-back blond hair, she wore gold hoop earrings and had a large tattoo of a leprechaun on her arm. “I had sensations. I could feel a lot of things–a lot of weird, creepy things,” she explained to me. “Like crabs were crawling on your toes, or like a slug was stuck to the side of your face, or like a spider was blowing on your head.”
Clougherty needed her medical condition checked before she could be sent to an inpatient psychiatric and detox facility. But that wasn’t easy to do. Although she gets her health care at the Neponset Health Center in Dorchester, some of her medical records were held in a special Boston-area computer system called BEST, for Boston Emergency Services Team, which was set up by BMC and mental-health agencies to keep track of psychiatric patients’ medications, hospitalizations, and histories. Petrozzi looked up Clougherty’s file. She saw a worrisome note from 14 years before: at the time, Clougherty had tested positive for tuberculosis. Since BEST is not integrated with the Neponset Health Center (and neither is BMC, though that’s in the works), Petrozzi had no easy way to see whether her patient might be sick and contagious. Without clarity in the record, doctors would have had to order a chest x-ray to rule out any signs of TB before releasing her.
Fortunately, Petrozzi and her colleagues were able to reach a Neponset staffer by telephone and confirm that Clougherty had had a clear x-ray within the previous year. But such improvisation is hardly a substitute for making electronic records readily available to the clinicians who need them. “Ideally, inpatient hospitalization admittance and discharge is supposed to provide a seamless transition from one milieu to the next,” Petrozzi said as we sat in her tiny, windowless office. On the wall hung a few reminders of other crises she deals with. A photocopied sheet of paper said, in bold letters: Please report all deaths to the New England Organ Bank–800-446-6362. She told me, “If you don’t have information–and it’s true of any level of care, but particularly in psychiatry–you are interfering in some way with the patient’s physical and mental well-being. You don’t want that to happen.”
The rancorous political debate over health-care reform tends to mask this kind of commonsense–and widely shared–understanding about the value of basic access to information. “The good thing about information is that most everyone can be in favor of it,” says Cutler, who recently coauthored a bipartisan report to Congress on the importance of properly deployed information technology in reforming health care. (It was also signed by a scholar at the conservative American Enterprise Institute.) “And if you look at the difference between the last time we looked at health-care reform, in the 1990s, and now, the single most important change is that the IT has changed. What everyone believes–not just left of center, not just right of center, but everyone–is that is now is the moment to seize that and really put it to work.”
David Talbot is Technology Review’s chief correspondent.