Rewriting Life
Manipulating Memory
Drugs that alter traumatic recollections offer new hope for treating anxiety disorders. They could also change the way we think about memory.
For psychologist Alain Brunet, the case is still astonishing. When Patrick Moreau first came into his office suffering from post-traumatic stress disorder (PTSD), the Canadian soldier, who had served as a United Nations peacekeeper in Bosnia, could hardly bear to recount the details of the day he was taken hostage in 1993. The memory–of kneeling on the ground with his hands on his head, legs shaking, a stark line of trees across the sky–aroused crippling fear that felt as fresh as it had 15 years before. The glimpse of a particular tree line through his windshield was enough to bring the memory rushing back, giving him such violent shakes that he would have to pull off the road.

But six months after participating in Brunet’s clinical trial, Moreau no longer meets the diagnostic criteria for PTSD. He still experiences some flashbacks, but they are less frequent and less intense. He can now talk calmly and openly about what happened. And all he did was take a blood-pressure drug after writing down the details of the traumatic experience.
“It seemed like science fiction,” says Brunet, a clinical psychologist at McGill University and the Douglas Institute in Montreal. “If someone is traumatized, you ask them to recall the memory, give them a pill, and the [emotional] strength of the memory is weakened.” The details of the trauma remain intact, but the emotional component of the memory appears to dissipate. Although larger studies are needed to assess the potential benefits of the treatment, preliminary findings are promising. Brunet has successfully treated PTSD not only in soldiers like Moreau but also in survivors of rapes and car accidents. “They are matter-of-fact,” he says. “When we ask them whether they have been thinking about the trauma, they raise their shoulders and say, ‘Eh, I am not thinking about it so much.’ It’s like it’s no longer an issue.”
Brunet’s potentially transformative treatment is based in part on a surprising experimental observation: the simple act of calling a memory to mind makes it vulnerable to alteration. Indeed, the right drug given at the right time can make parts of it disappear altogether. If different drugs are delivered to specific parts of the brain, lab animals will explore cages they’ve been conditioned to fear, drink fluids once associated with certain sickness, and ignore sights and sounds that previously led them to expect cocaine or other pleasure-inducing drugs. Humans, too, can be tricked into scrambling their memories in specific ways. For example, if people learn a list of words soon after recalling a previously learned list, they tend to forget the old list or incorporate those words into the new one. The memory of the old list remains intact if people aren’t reminded of it just before learning the new one. And it’s always the old list that gets incorporated into the new, not the other way around.
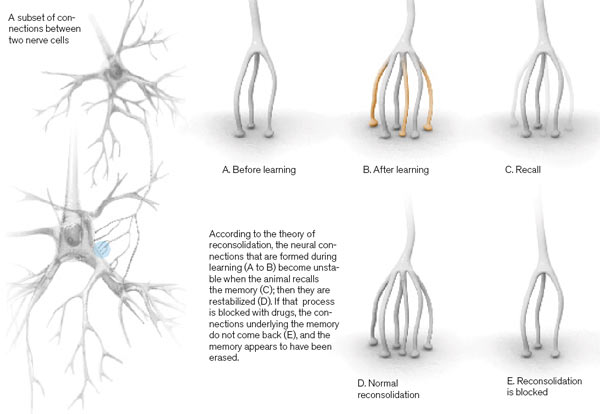
Brunet and others believe that this phenomenon has to do with a process called memory reconsolidation. The idea is that after someone calls up a memory, it has to be stored in the brain anew. During this process, the memory is in a changeable state. The concept of reconsolidation is still controversial among neuroscientists. But if the theory is correct, and if researchers can figure out just what happens to brain cells and the connections between them when a memory is recalled, it could help answer one of the biggest questions in neuroscience: how memories are physically saved and updated in the brain. It could also explain the malleable nature of memory. “It gives us a new perception of a component of memory we didn’t understand before–how the imperfectness of recall may come about,” says Eric Kandel, a neuroscientist at Columbia University and winner of the 2000 Nobel Prize in medicine.
Brunet is one of the few people studying reconsolidation in humans. In his trials, he administers a medicine called propranolol, which is already used to treat high blood pressure. It decreases blood pressure by blocking the action of epinephrine, a stress hormone, in the peripheral nervous system. But it also blocks the hormone in the amygdala, a part of the brain that plays a crucial role in storing the emotional components of memory. If Brunet proves that this treatment can weaken the grip of painful memories, he won’t just have found an alternative to behavioral therapy and existing drug treatments for PTSD, none of which work for everyone. He will also have demonstrated that it might be possible, through drug treatment, to fundamentally and precisely alter memories beyond the confines of the lab. The implications are immense. Brunet’s general approach to understanding memory could be used to treat a variety of anxiety disorders and addictions.
A Window of Vulnerability
At the simplest level, a memory is thought to be stored in the brain by a specific, well-connected circuit of nerve cells linked by junctions called synapses. New memories are formed when synapses form or existing synapses grow stronger as the brain processes events.
One of the tenets of modern neuroscience is that it takes time for these memories to become permanent–a process dubbed consolidation. In the 1960s, scientists subjected rats to various treatments that block normal brain signaling (for example, electroconvulsive treatment, or ECS, disrupts electrical signals by inducing seizures). The results showed that very new memories could easily be kept out of permanent storage. But if the disruptive treatments were administered a day or so after the new memory was created, they had no effect. Once a particular memory becomes resistant to interference, it is regarded as consolidated.
The first hint that long-term memories could be made malleable came in the 1960s too, just as the idea of consolidation was gaining ground. Through experiments similar to those that defined the time window for consolidation, scientists discovered that ECS could disrupt even an old memory in animals, if the animal was reminded of it first. To start, the researchers would condition rats to fear a particular sound by giving them a mildly painful shock every time they heard it. The animals would eventually freeze in fright on hearing the sound: the painful memory had been consolidated. But when the rats were given ECS treatment just after the memory was triggered by playing the sound, the fearful link between the sound and the shock was lost forever. Because this rather confusing finding conflicted with the dominant theory that consolidated memories are permanent, it was pursued only briefly, and then largely forgotten for the next 25 years.
Over the next few decades, scientists came up with more precise ways to study the molecular underpinnings of memory and consolidation. In 1999, for example, researchers in neuroscientist Joseph LeDoux’s lab at New York University found that injecting a drug that blocks protein synthesis directly into part of the brain disrupted consolidation of new memories. Researchers proposed that when the right proteins aren’t produced, nerve cells can’t make the connections that underlie memory formation at a cellular level.
In 2000, Karim Nader, then a postdoctoral researcher in LeDoux’s lab (he is now an associate professor at McGill), published a paper showing evidence that the same drug treatment could also erase long-term memories that had recently been recalled–a major new challenge to the prevailing views about consolidation. Nader, who was new to memory research but had access to neuroscience not available in the 1960s, outlined a specific theory explaining this observation. He proposed that recalling a memory actually causes the synapses encoding that memory to weaken or even to come apart. The molecular structure of the memory–the series of synapses in which it’s stored–is then re-formed, or reconsolidated, to make it stable once again.
When Nader presented his work in 2001 to a crowded lecture hall at the annual meeting of the Society for Neuroscience, the field’s premier academic gathering, he faced outright disbelief from some leaders in the field. “It caught the attention of lots of other neuroscientists, because some had taken the view that once consolidation had been completed, it couldn’t be dislodged,” says David Riccio, an experimental psychologist at Kent State University in Ohio, whose own research in the 1970s had challenged the consolidation model.
It makes sense that the brain, in order to take in and store new information, would need to have some flexibility in the way it stores old memories. But does this really mean that when an old memory is recalled, the brain must dismantle the synaptic structure underlying the memory and then form it again? “Reconsolidation strikes me as a woefully inefficient way to make memory work,” says Ralph Miller, a behavioral neuroscientist at the State University of New York at Binghamton, who was also involved in the 1960s consolidation debate. “My own best guess is that every time we recall a memory, we lay down new versions.” In this model, the existing memories would remain intact, but they would be integrated with the new ones or superseded by them–meaning that the old memories would still exist in the brain but would be less accessible than the new ones.
Despite such doubts, evidence for the theory of reconsolidation is piling up. One experiment, for example, has found that blocking the molecules involved in protein degradation, which is necessary to break down synapses, makes animals forget a memory after it’s been recalled. The finding suggests that reconsolidation–which couldn’t happen without the initial breakdown–is the only way to explain why such memories don’t normally vanish.
A more recent experiment, published late last year, begins to get at the purpose of reconsolidation: it may help update memories, integrating them with information about related newer experiences. Jonathan Lee, a neuroscientist at the University of Birmingham in the United Kingdom, trained rats to fear a certain chamber by shocking them soon after they entered it. More training strengthened the association; evoking the memory made these rats freeze for longer than rats trained over just one day. Then Lee blocked a protein required for the consolidation of new memories; in a second set of animals, he instead blocked a gene that is critical to reconsolidation. He found that blocking consolidation did not interfere with the strengthening of the memory, while blocking reconsolidation did. This suggests that reconsolidation, not consolidation, is what’s important in strengthening memories, which is one way of updating them. “Learning something for the second time seems to use the reconsolidation mechanism,” says Lee. “Learning is strengthened by going back to the initial memory.”
Lee’s work implies that new versions of a memory are not laid down on top of a surviving old version when the memory is updated, as Miller’s alternative explanation suggests. Rather, the instability of a recalled memory may be crucial to the updating process. “Our assumption is that when you activate a memory, you set it up to be updated,” says Lynn Nadel, a neuroscientist at the University of Arizona. “You make [the memory] fragile so that it is open to being changed.”
Still, many questions about reconsolidation remain. Several experiments have shown that under some circumstances, erased memories can come back, suggesting that the initial memory was not truly erased. Meanwhile, both the age of the memory and its initial strength sometimes seem to affect how malleable it is: older memories, for example, can be more resistant to alteration, though that’s not always the case. Some scientists see these limitations as evidence that Nader’s theory of reconsolidation doesn’t adequately explain recall-induced forgetting. But it may be that reconsolidation happens only under specific conditions or with specific types of memory, while other mechanisms are used to update memory in the other situations. What we don’t yet understand is which types of memory are vulnerable to alteration and under what circumstances, says Jerry Rudy, a neuroscientist at the University of Colorado in Boulder, the author of The Neurobiology of Learning and Memory. Other researchers are now exploring whether reconsolidation is a fairly limited occurrence or one that’s fundamental to memory as we conceive of it.
Even as the evidence for reconsolidation accumulates, the idea that the neural connections underlying our memories routinely come undone has some disturbing implications. Among the most significant is that our memories are vulnerable to inadvertent alteration. If the brain went to the trouble of storing a memory, why would it then have a mechanism that makes it so easy to erase? “It just doesn’t make sense that a cherished childhood memory should become vulnerable to erasure,” says Larry Squire, a neuroscientist at the University of California, San Diego. That vulnerability also has positive implications, however: the potential to weaken bad memories.
Painful Pasts
Brunet’s office at the Douglas Institute in Montreal, its bright-orange walls adorned with paintings and greenery, emanates a cheeriness in stark contrast to the grim nature of his research. He decided to focus his career on PTSD while still a college student in the late 1980s at L’Ecole Polytechnique in Montreal, after a gunman entered an engineering class there and killed 14 women in a shooting rampage.
New treatments for PTSD are sorely needed. A recent study showed that about 15 percent of U.S. combat troops returning from the wars in Iraq and Afghanistan show signs of the disorder. And while some effective treatments exist, they consume a lot of time and resources, and they don’t work for everyone.
Developing better therapies is easier, of course, if we know what causes the problem in the first place. One hypothesis holds that PTSD stems from a memory that is too strong, burned into the brain by hormones released in times of stress. These hormones, which surge as part of the body’s fight-or-flight response, activate cells in a part of the brain responsible for the emotional component of memory. In an evolutionary context, enhancing the storage of frightening memories makes sense: the more vividly you remember scary situations, the more likely you may be to stay away from them in the future. But in PTSD, that process appears to have gone awry, producing pathologically powerful memories that are triggered by the smallest reminder. Researchers have had some success in preventing the formation of these supermemories by dampening the stress response soon after a trauma: Brunet and his colleague Roger Pitman, a psychiatrist at Harvard Medical School, have both shown that patients given epinephrine-blocking propranolol in the emergency room are less likely to develop PTSD. “The idea was that if you could decrease the release of stress hormones following a trauma, you could influence the saliency of that memory in the future,” says Brunet.
This prevention strategy might work well in a military context, where everyone involved in a particular combat event could be given the drug, but it’s not ideal for civilians. The time window for treatment is limited, and not everyone who experiences a trauma will rush to the ER. “Even treating people four to six hours after the trauma may be too late,” says Pitman. If a treatment can’t help them, it certainly can’t help people who already have PTSD.
In 2004, Pitman–having learned of Nader’s work–had another idea: to use propranolol to try to mimic animal research on reconsolidation, much of which has focused on fear memories. Researchers studying reconsolidation had previously suggested that blocking the reconsolidation of traumatic memories in people might help make these memories less troubling. Propranolol, it turns out, acts on the part of the brain that is central to the emotional component of memory–the same area targeted in Nader’s rodent research. (Factual components of memory are stored in a different part of the brain.) By reactivating the patients’ memories, Pitman proposed, “we could reopen the window of opportunity and get a second chance to treat PTSD.”
A pilot study of the treatment found that propranolol did seem to soothe the anxiety provoked by patients’ traumatic memories, long after the drug itself was gone from the body. In the study, patients wrote down their recollections of the trauma and then took a single dose of propranolol or a placebo. Those who received the drug were much calmer–as measured by heart rate and skin conductance–when reading a script of their stories a week later.
A larger study of about 60 people is now almost complete. Preliminary findings show a 40 to 50 percent improvement in self-reported symptoms among those taking the drug. At the end of the trial, nearly two-thirds of the patients in one of the groups taking propranolol no longer met the criteria for PTSD. The same was true for less than 10 percent of control patients.
Brunet pulls up a graph on his computer screen, its downward-slanting line reflecting the continued decline in the propranolol recipients’ PTSD symptoms over the five weeks of the study. “We’re seeing at least as good, if not better, results than people get with exposure treatment–and in much less time,” he says. (In exposure treatment, one of the most common types of behavioral therapy for PTSD, patients repeatedly recall the details of their trauma with a therapist in a safe environment, eventually learning to dissociate the extreme fear from the details of the event.) And patients were still doing well four months after treatment, even though relapse is fairly common in PTSD therapy.
Though the results are preliminary (the treatment must still be tested in a proper double-blind study, in which neither patients nor physicians know who is getting the drug rather than the placebo), the work has attracted great interest. The U.S. Department of Defense has awarded Brunet, Pitman, and Nader a $7 million grant over four years to identify additional existing drugs that can target reconsolidation more effectively than propranolol. The study will focus on drugs that are already on the market, which means they are already deemed safe and can be tested in PTSD patients without additional animal testing. Pitman and his colleagues are currently testing opioids such as morphine in rodents. His group has also seen preliminary success in rodents with RU-486, the abortion pill; in addition to affecting progesterone, a hormone involved in pregnancy, the drug blocks the action of chemicals called glucocorticoids, which are found in the amygdala and play a role in the emotional aspect of memories.
Thumbing through a thick stack of grant applications on his desk, Brunet says he thinks that targeting reconsolidation will alleviate a range of problems beyond PTSD. “We might have discovered a new way of treating mental disorders,” he says. “There are several disorders that have at their core a problem with emotional memories.” Specifically, he says, “many types of addictions, while physiological, also include a psychological component.”
While the role of memory may not be an obvious consideration in treating drug abuse, the sights, sounds, and smells that remind addicts of their habit are a strong trigger for relapse. Brain imaging studies demonstrate that if an addict is shown a trigger, such as a needle, the part of the brain associated with drug use immediately fires up. Psychiatrists have tried exposure therapy to rid addicts of these intrusive memories, with little success. However, studies show that blocking the reconsolidation of drug-linked memories works remarkably well in animals. In fact, says Barry Everitt, a neuroscientist at the University of Cambridge in England, “it’s the only thing that works well.”
True Identity
Easing the pain of difficult memories sounds like a dream come true, perhaps even for people who don’t suffer from anxiety disorders. But the idea also raises concerns. Such memories, after all, are an integral part of a person: frightening, sad, perhaps life-changing moments make up important chapters in the stories of our lives. We might not be the same if remembering these events felt no more emotional than recalling a trip to the grocery store.
But Brunet points out that he is trying to bring PTSD patients’ memories into a normal emotional range, not blunt their power altogether. “Months after a breakup, when the pain is beginning to fade away, do you feel that you have lost something?” he asks. “Of course not. That’s the fate of normal emotional memory.” In PTSD, on the other hand, the memory is as painful and crippling as if the events had occurred yesterday, making it difficult to lead a normal life. He doesn’t think that using propranolol to render these memories bearable would create any unique potential for abuse as a way to dull the regrets, fears, and embarrassments of everyday life; people already use alcohol and other drugs for such purposes.
The ethical worries may stem in part from a misunderstanding about the level of control that scientists have over memory. Researchers can manipulate memories only in very subtle ways. It’s not possible to erase a web of interconnected memories, or to program people with substantial new memories. (Research into false memories and eyewitness testimony suggests that a memory can be subtly influenced: someone who has witnessed a car accident, for example, may estimate different speeds for the car depending on whether they are asked how fast they saw it “smash” or “bump” into a tree. But these changes are minor tweaks to existing memories.)
It’s still too early to predict the ultimate impact that drugs and other treatments targeting reconsolidation will have on human memory. But for now, the power to block reconsolidation is giving scientists a new tool to probe the brain’s storage system. Nader’s next step is to use his research on reconsolidation to study how the brain files memories. If rats are taught two different associations–say, pairing a light with a shock and a sound with a shock–does blocking the reconsolidation of one memory affect the other? Experiments like this will begin to shed light on whether memories are stored according to when they were formed, the context in which they were formed, or other variables. Bit by bit, the answers to such questions should help unravel one of the most enticing mysteries of the mind.
Emily Singer is Technology Review’s senior editor for biomedicine.
